
1. Give an example of a research question for investigating racial/ethnic health disparities where: [1] SES is a confounder; [2] SES is an effect modifier; [3] SES is a mediator. Briefly discuss the interpretations/implications of each approach as it relates to understanding health disparities by race/ethnicity.
Using examples taken from a study I am currently working on, I found this to be a helpful, yet challenging question. In the examples below, I am making several assumptions about what is included in SES, and do not directly include race/ethnicity, but have attempted to explain the interpretation/implications with each example.
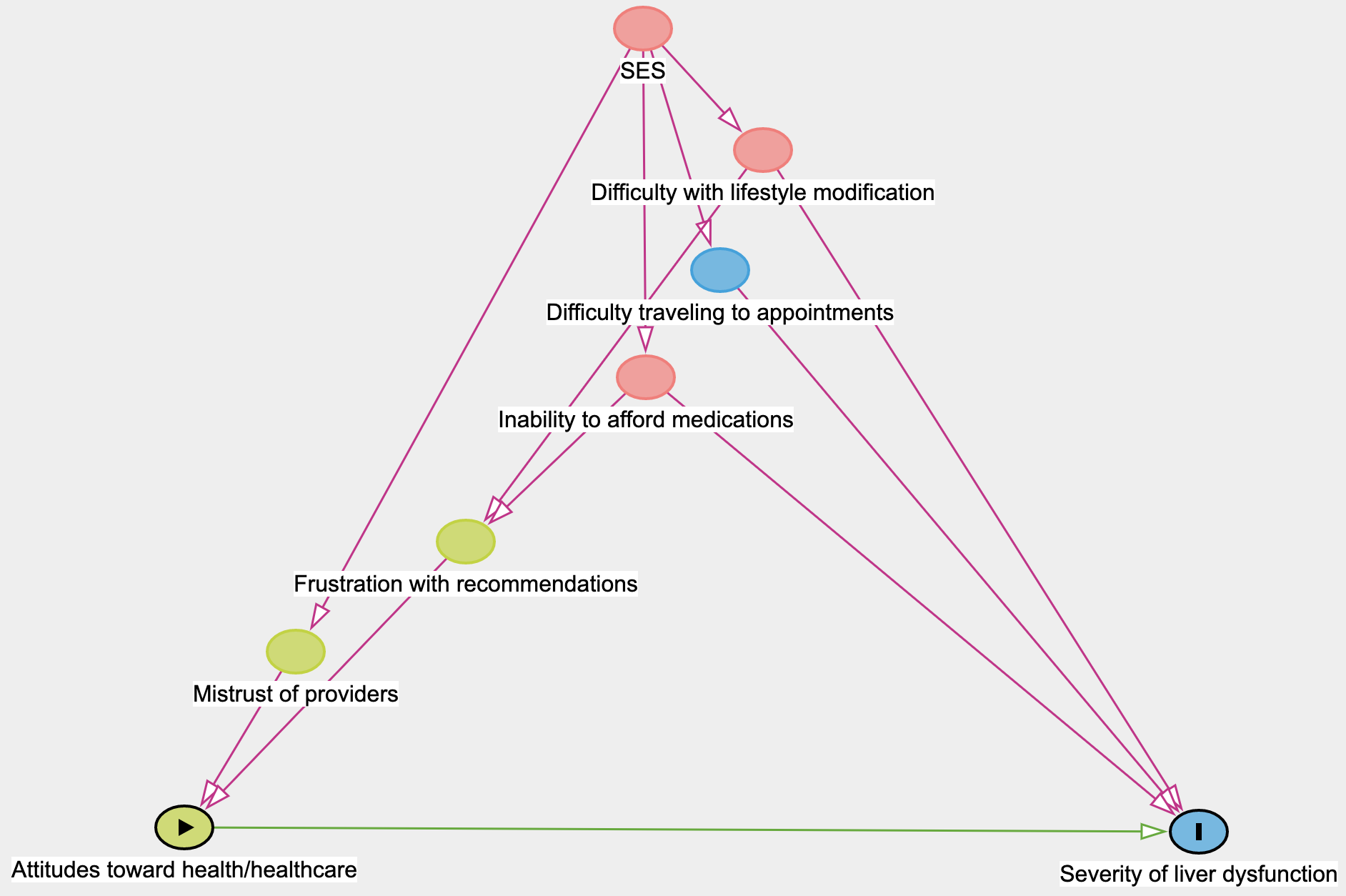
SES as a confounder: we are looking at our patients’ attitudes toward healthcare and their diagnosis of fatty liver disease, and in this example, interested to see how those attitudes impact liver dysfunction over time. Since fatty liver disease is currently managed via lifestyle modification, patients must actively participate in their care, and attitudes toward the diagnosis (particularly because it is often asymptomatic) and the health system in general, is very important. With this question, we can stratify the responses by race/ethnicity to see if there are any patterns in our patient population. If these exist, educating providers of these differences and brainstorming ways to implement changes to the structure of our clinic or the individualized counseling may be helpful.
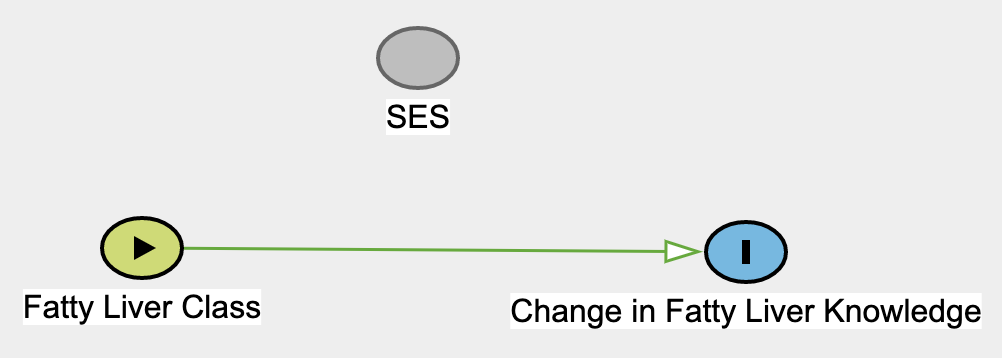
SES as an effect modifier: we are measuring the change in knowledge of our patients pre and post attendance of free fatty liver class taught by our providers. SES is an effect modifier in this example because I think that based on SES, patients will likely benefit differently from the class. For example, patient of higher SES, if that also correlates to higher health literacy, may already score well in knowledge on the pre-education survey, and therefore their knowledge score will not change. Perhaps patients with lower SES will benefit most significantly from the class as they have lower initial knowledge of fatty liver disease, but they are able to learn a lot from the course; their change in knowledge will increase more. Patients with very low SES – possibly lower education level if they are illiterate or have undiagnosed mental health conditions, learning disabilities, etc, - they may start with very little knowledge, but then also may not benefit from a class. Their change in knowledge may not change at all, and therefore they may benefit from one-on-one education. This is how level of SES modifies the effect of the fatty liver class on knowledge.
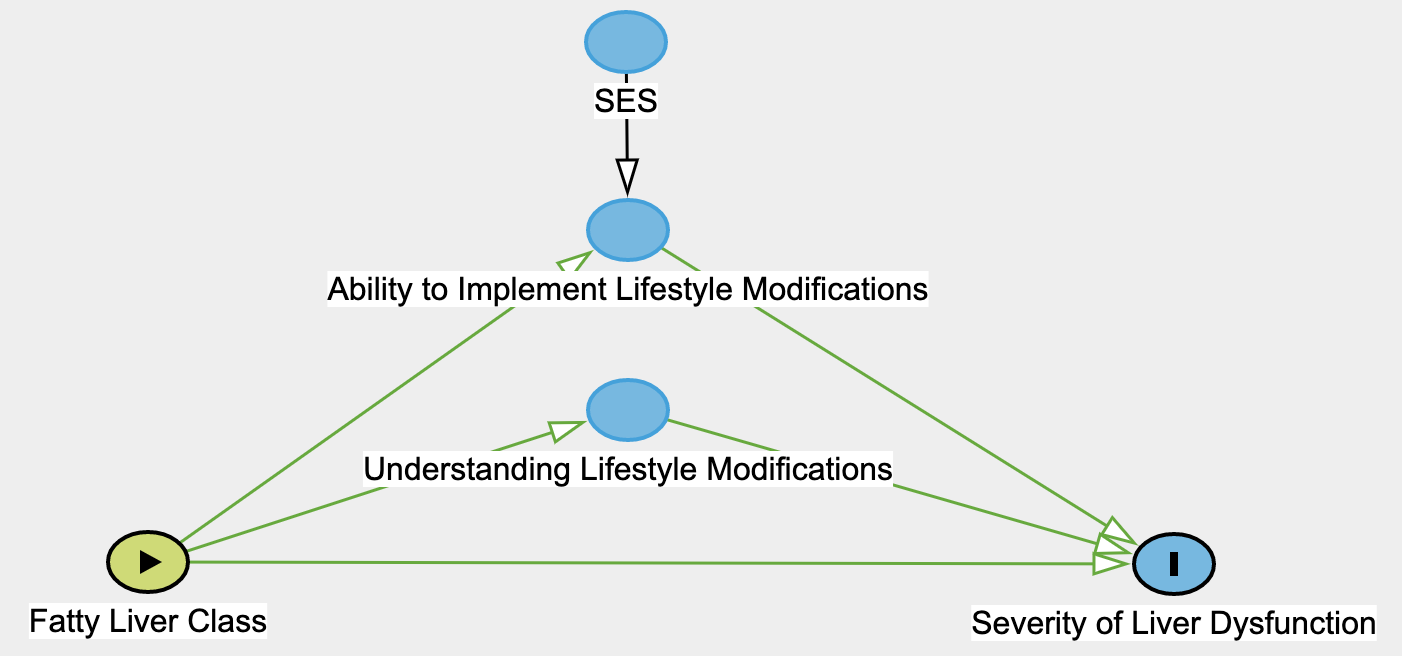
SES as a mediator: in this example, I am interested in looking at our intervention of the fatty liver class on the outcome of severity of liver dysfunction. We are assuming the fatty liver class affects the outcome in several ones, but one major way is through a better understanding of what lifestyle modifications are beneficial for fatty liver disease. This is drawn as a mediator above. However, just because someone understands the recommended lifestyle modifications does not mean they can easily make those changes. I have included ability (or rather barriers) to implementing lifestyle changes as another mediator, and SES has a direct relationship on this. Again, understanding how SES correlates with race/ethnicity in our study population will be helpful and may be one way we can tailor our class or individual patient counseling in clinic to help our patients achieve better outcomes when it comes to their liver disease.
2. Describe a potential effect modifier, mediator, or contextual variable (for definition of contextual variable, see Diez-Roux reading) for an association of interest to you and relevant to health disparities. For example, for investigating the association between education and hypertension, I might be interested in evaluating whether the association between years of education and hypertension is different for Black men than for White men. Describe how you would study whether this relationship exists.
I am interested in SES as an effect modifier on change in knowledge pre- and post-fatty liver education course, as listed above. However, I am also interested to see how attitudes intertwine with this relationship. I believe if a relationship is seen between attitudes toward fatty liver disease diagnosis and change in knowledge after the fatty liver education class, I would be interested in conducting focus groups with patients to better understand this relationship, and to clarify if and how SES plays a role. It would also be helpful to understand if SES is an effect modifier on change in knowledge in the way I described above, if that is partially occurring due to differences in attitudes toward healthcare and the diagnosis of fatty liver disease. I think the only way to understand these complex interactions would be through focus groups.