1. Write a paragraph describing the extent to which an socioecological framework incorporating issues related to social determinants has been applied to your area of research. Are there opportunities for improving our understanding of or approach to disparities in your area with a greater emphasis on a socioecological framework?
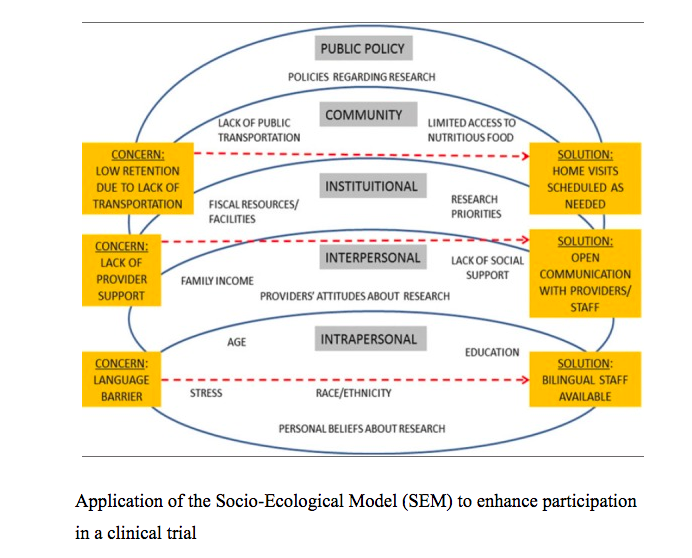
I am interested in disparities across the cancer care continuum. The scope of my most recent work has related to inequity in cancer clinical trial recruitment. Prior investigators have explored a socio-ecological model (SEM) as a framework for improving recruitment and retention among underrepresented populations. Salihu et al described SEM as a model that makes the assumption that an “individual’s behavior is integrated in a dynamic network of intrapersonal characteristics, interpersonal processes, institutional factors, community features and public policy. The model assumes that the interactions between individuals and their environment are reciprocal.” (Salihu, 2015). These investigators developed the conceptual model attached to this post. This framework reveals that the complexity that underpins the problem of clinical trial recruitment and retention. A vast literature exists exploring the bottom and top layers: intrapersonal and public policy. However less is known about interpersonal, institutional, and community contexts that contribute to disparities in whom clinical trials serve. Qualitative researchers, ethnographers, and social scientists at our own institution are adding to the literature on interpersonal dynamics (Drs. Galen Joseph, Daniel Dohan, Nancy Burke, Celia Kaplan). On an institutional level, other investigators and clinicians have described the concept of a health literate organization (Brach et al, 2012). This notion gets at the institutional level – in a fundamental way. However it is a cross cutting concept that also touches on all pillars of the SEM model. The SF CAN initiative which is a city wide effort to mitigate disparities is really targeting the community level of this model. My research has been largely entrenched in the interpersonal level. I am particularly interested in the direct out of pocket costs patients assume while enrolled in trials. I am also designing an intervention that is aimed at helping low health literacy patients navigate cancer clinical trials. In an effort to develop this intervention, I have to be versed on all levels of this paradigm. In summary, there has been, and continues to be, a need to apply the SEM framework in order to better understand and address disparities in cancer clinical trial recruitment.
2. In the WHO reading, A conceptual framework for action on the structural determinants of health, the authors describe structural stratifiers (e.g. income, education, etc) and intermediary determinants such as material and psychosocial circumstances. Pick 3 of these factors (at least one structural and one intermediary). Explain why you chose the factors (might use Braveman article to provide justification) and describe how each could be an important determinant of a health outcome of your choosing. The association could be reported in published research or it could be your hypothesized relationship. Consider whether how these factors might function over the lifecourse and/or intergenerationally.
When it comes to a problem such as clinical trial recruitment and retention in the United States, countless structural and intermediary determinants influence the observed disparities. For one, today more than ever we are well aware of race/ethnic disparities in socioeconomic position (structural determinant) and that an individuals ability to transform their SES is influenced by governance, macroeconomic, social, and public policies.
For example, lets think about immigration status and clinical trials. We know that a person living in the United States under DACA, facing concerns for deportation and family separation is less likely to engage in an investigational study because they have concerns that extend far beyond their cancer. We know from important ethnography (The Good Study Patient by Drs. Dohan and Joseph), that implicit bias influences what patients are offered clinical trials in the first place. Would a physician really offer a clinical trial to a patient who has a tenuous immigration status? Unlikely.
Now intermediary determinants of SDH such as material circumstance (wage, food security) are obvious contributors to disparities in clinical trial. Researchers at Dana-Farber at the Cancer Care Equity Program (CCEP) have attempted to mitigate this contribution to disparities with financial support to patients of low income (Nipp, 2016). They have observed, naturally, that if you provide financial support to off set the direct costs associated with clinical trials (e.g. travel, lodging) you are better able to recruit from low income populations.
The intermediary determinant of behavior and biology is also a natural contributor to disparities in clinical trials. For example, a patient that is less adherent to standard therapy would less likely be enrolled in a clinical trial. This has been demonstrated in ethnographic research as well. Patients who are better able to follow protocol and have higher health literacy (which is connected with the education level - a Structural Determinant) are more likely to be enrolled.
Honestly, I think the lines between structural and intermediary determinants of SDH are blurred. Education affects behavior. Biology may affect income. If you have a more aggressive disease you may be less likely to work. Material circumstance is tied to occupation. However I think the conceptual framework is a good foundation for thinking about investigating problems and by extension designing targeted interventions.