
1. Write a paragraph describing the extent to which an socioecological framework incorporating issues related to social determinants has been applied to your area of research. Are there opportunities for improving our understanding of or approach to disparities in your area with a greater emphasis on a socioecological framework? Consider drawing a DAG or a socioecological model (like the one shown in class for obesity) to illustrate your point (you can take a picture to post on the forum).
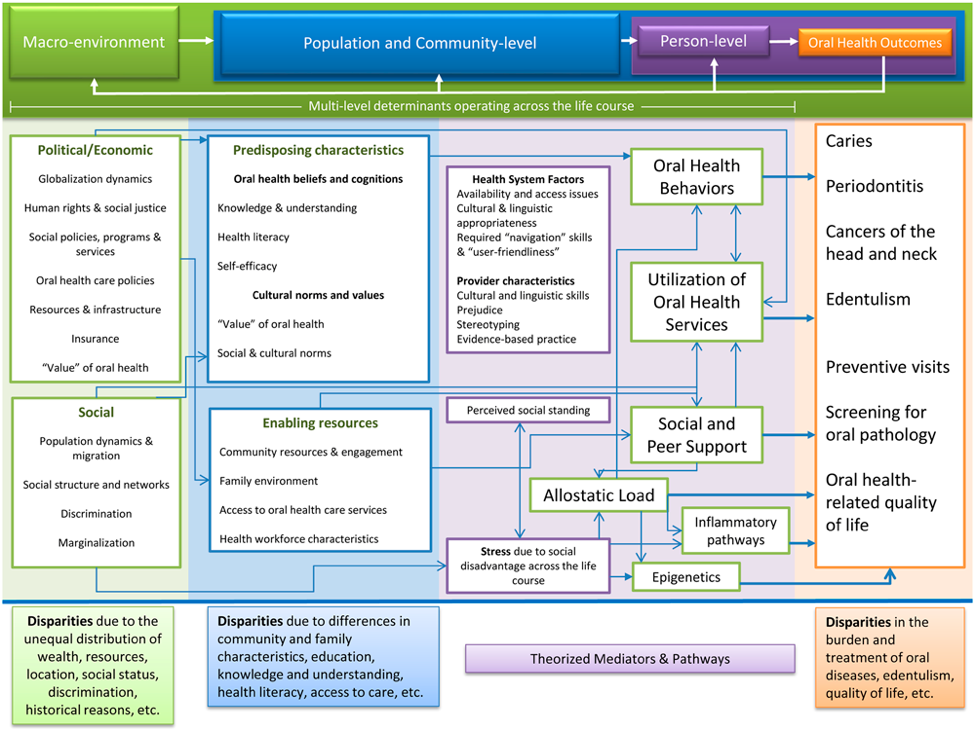
My area of interest in research is oral medicine, which is the intersection between medicine and dentistry, with a special focus on premalignant lesions of the oral cavity. Oral health disparities are most commonly reported for caries, chronic periodontitis, and cancers of the head and neck. The mouth and oropharynx are among the ten most common sites affected by cancer worldwide, but global incidence varies widely. Five-year survival rates exceed 50% in only the best treatment centers. Causes are predominantly lifestyle-related: Tobacco, areca nut, alcohol, poor diet, viral infections, and pollution are all important etiological factors. In the figure 1 Lee and Divaris present a proposed framework for conceptualizing and addressing these oral health disparities (Lee and Divaris, 2014). Although one model cannot possibly include all determinants, pathways, and oral health outcomes, it represents a detailed scheme of the current state of knowledge in the oral health disparities. This model is based on a modification of Andersen’s behavioral model and builds upon previous work on the multi-level influences of oral health (Patrick et al., 2006), as well as oral health disparities (Watt and Sheiham, 2012). The majority of cases of oral cancer occur without the patient or the managing physician being aware of any pre-existing lesion, despite a probable background of systemic predisposing factors. If we refine this model and integrate the variables that can identify these premalignant lesions, it could generate opportunities for early intervention: on a population basis, as detection targets and activators for health promotion; and based on the patient, for the intervention of habits, nutritional support and surveillance for malignant transformation. There is no evidence of the benefits of such interventions, and there is a need to investigate effects on natural history and outcomes.
2. In the WHO reading, the authors describe structural stratifiers (e.g. income, education, etc) and intermediary determinants such as material and psychosocial circumstances. Pick 3 of these factors (at least one structural and one intermediary). Explain why you chose the factors (might use Braveman article to provide justification) and describe how each could be an important determinant of a health outcome of your choosing. The association could be reported in published research or it could be your hypothesized relationship. Consider whether how these factors might function over the lifecourse and/or intergenerationally..
Behaviors factors: Oral cancer, traditionally a disease of elderly men with a history of chronic exposure to the carcinogenic effects of tobacco and alcohol (Adeyemi, Olusanya and Lawoyin, 2011). Most cases occur in the fifth to seventh decades of life, probably because long exposure to tobacco, alcohol, and poor nutrition is needed for interaction with other agents to trigger malignant transformation.
Education and Income: There is a marked association between oral cancer, education and income (Winn et al., 2015). These factors may reflect exposure to harmful physical environments and agents which could increase the risk for oral cancer. It may also determine access to health services, social facilities and to the affordability of quality food.
Race/ethnicity. The strongest evidence of differences in oral cancer mortality comes from the USA. There, death rates from cancer of the mouth and pharynx among blacks in 1987 (5.7 per 100 000) were higher than among whites (3.4 per 100 000). Analysis of the NCI’s SEER data showed that most of the increased risk of death from mouth cancer in Afro-American was due to more advanced stage of disease, and differences in the type of treatment they received (Scully and Bedi, 2000).
Adeyemi, B. F., Olusanya, A. A. and Lawoyin, J. O. (2011) ‘Oral Squamous Cell Carcinoma, Socioeconomic Status and History of Exposure to Alcohol and Tobacco’, Journal of the National Medical Association. Elsevier, 103(6), pp. 498–502. doi: 10.1016/S0027-9684(15)30364-3.
Lee, J. Y. and Divaris, K. (2014) ‘The Ethical Imperative of Addressing Oral Health Disparities’, Journal of Dental Research. SAGE PublicationsSage CA: Los Angeles, CA, 93(3), pp. 224–230. doi: 10.1177/0022034513511821.
Patrick, D. L. et al. (2006) ‘Reducing Oral Health Disparities: A Focus on Social and Cultural Determinants’, BMC Oral Health. BioMed Central, 6(Suppl 1), p. S4. doi: 10.1186/1472-6831-6-S1-S4.
Scully, C. and Bedi, R. (2000) ‘Ethnicity and oral cancer.’, The Lancet. Oncology. Elsevier, 1(1), pp. 37–42. doi: 10.1016/S1470-2045(00)00008-5.
Watt, R. G. and Sheiham, A. (2012) ‘Integrating the common risk factor approach into a social determinants framework’, Community Dentistry and Oral Epidemiology. John Wiley & Sons, Ltd (10.1111), 40(4), pp. 289–296. doi: 10.1111/j.1600-0528.2012.00680.x.
Winn, D. et al. (2015) ‘The INHANCE consortium: toward a better understanding of the causes and mechanisms of head and neck cancer’, Oral Diseases. John Wiley & Sons, Ltd (10.1111), 21(6), pp. 685–693. doi: 10.1111/odi.12342.