
1. Give an example of a research question for investigating racial/ethnic health disparities where: [1] SES is a confounder; [2] SES is an effect modifier; [3] SES is a mediator. Briefly discuss the interpretations/implications of each approach as it relates to understanding health disparities by race/ethnicity.
I think one of the most difficult aspects of research so far is that the DAG can be written many different ways and the way the dag is written can truly affect how the data is analyzed. Currently I am wrestling on research project that is looking at HTN control in racial ethnic minorities. I think in the dag model, SES could be considered a confounder, effects modifier, or even a mediator depending on how the investigation team considers how SES falls. For instance, SES could be a confounder that causes more stressful situations in African American populations and causes higher blood pressure. SES could be considered an effects modifier that changes based on race, or it could be a mediator between raceàSESàHTN control. I could see them all as being a plausible dag diagram. This has actually been one question I have had when approaching research, which one do you choose? Do you go on a fishing expedition, blinding casting the rod in different locations to try and find confounding, effects modification, or mediation? To me, this doesn’t seem to be the right path. Even if a metaphorical fish is caught it could just be due to luck. Fishing should be done with a carefully planned purpose, which comes down to carefully considering the DAG for association, confounding, effects modification, and mediation.
Which gets me back to the second question, the interpretations/implications of considering SES can have a large role in understanding the health disparity. If you consider SES to be a confounding factor that affects both race and HTN, then this could lead to research that concludes that by elevating the SES of this population the association would be alleviated. Furthermore, if you consider SES to be an effects modifier that interacts with race on different levels, this could point to different interactions depending on the race and ethnicity, which could further entrench the differences between races/ethnicities and could potentially have sociologic fallacies present. Finally, if you consider SES a mediator for HTN control for those of different races, it leads to implications that by being a certain race, race causes your SES and thus the health outcome.
Thinking about the way the DAG is drawn and the meaning for health disparities truly changes with each interpretation. Great thought must be invested when approaching SES and its implication on race/ethnicity and health outcome.
2. Describe a potential effect modifier, mediator, or contextual variable (for definition of contextual variable, see Diez-Roux reading) for an association of interest to you and relevant to health disparities. For example, for investigating the association between education and hypertension, I might be interested in evaluating whether the association between years of education and hypertension is different for Black men than for White men. Describe how you would study whether this relationship exists.
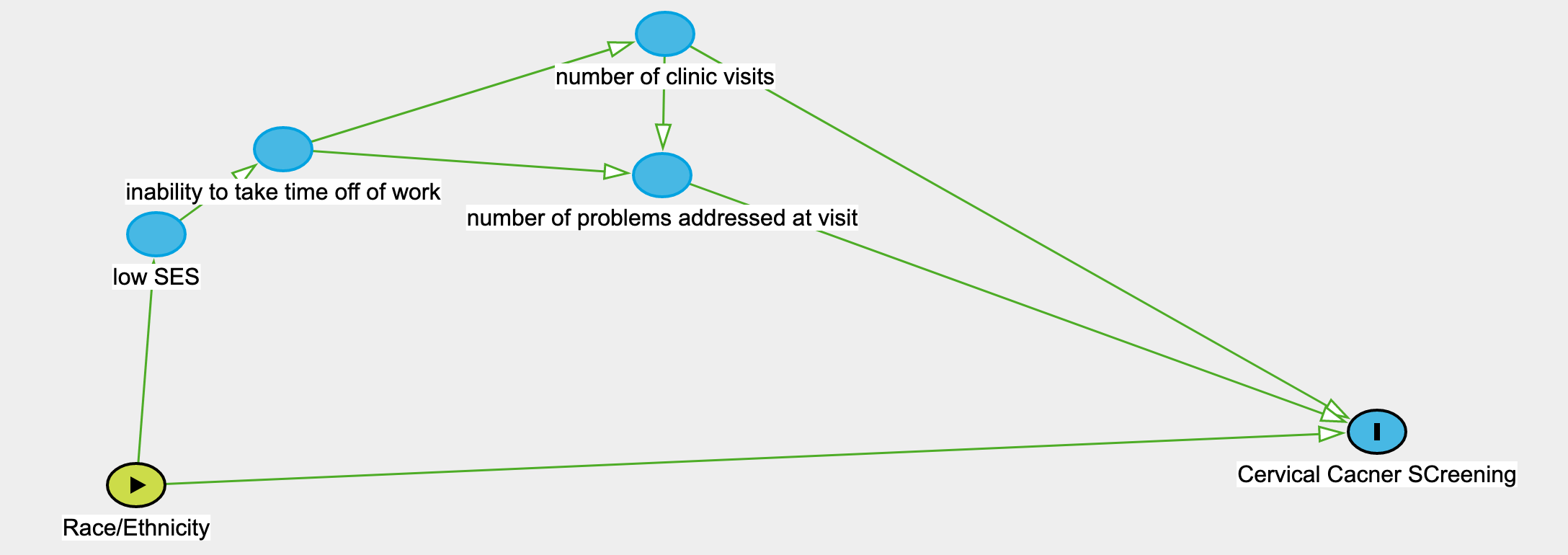
Going back to my cervical cancer research, I think a contextual variable that could be associated with my interest in health disparities in cervical cancer screening could be the average number of clinical visits per racial/ethnic group/year or number of diagnoses codes per visit per racial/ethnic group, it could also be broken down into neighborhood taking out the aspect of race/ethnicity entirely. Perhaps in neighborhoods with lower SES and non white populations, patients are not able to make it to as many appointments and come to clinic with the goal of addressing acute issues rather than preventative care. I could see this being reflected in number average number of clinic visits/year or average numbers of ICD-10 diagnosis addressed at a visit. These would both be able to be pulled from EHR data. Looking at EHR you might find that lower SES patients have longer intervals between visits, have many acute ICD-10 diagnosis codes, with few preventative care diagnoses.
3. Respond to one other person's post on the forum with a comment or suggestion
Responded to Leslie Suen’s post