
1. Give an example of a research question for investigating racial/ethnic health disparities where: [1] SES is a confounder; [2] SES is an effect modifier; [3] SES is a mediator. Briefly discuss the interpretations/implications of each approach as it relates to understanding health disparities by race/ethnicity.
Research question: Does mortality in patients with rheumatoid arthritis-associated interstitial lung disease (RA-ILD) differ by race/ethnicity?
Recognizing that “SES” could mean many things (income, education, etc), I have chosen one level of SES for each example:
SES as a confounder:
In thinking of race and ethnicity as social constructs, the DAG below represents the association of race and ethnicity and mortality in RA-ILD with social constructs as a confounder:
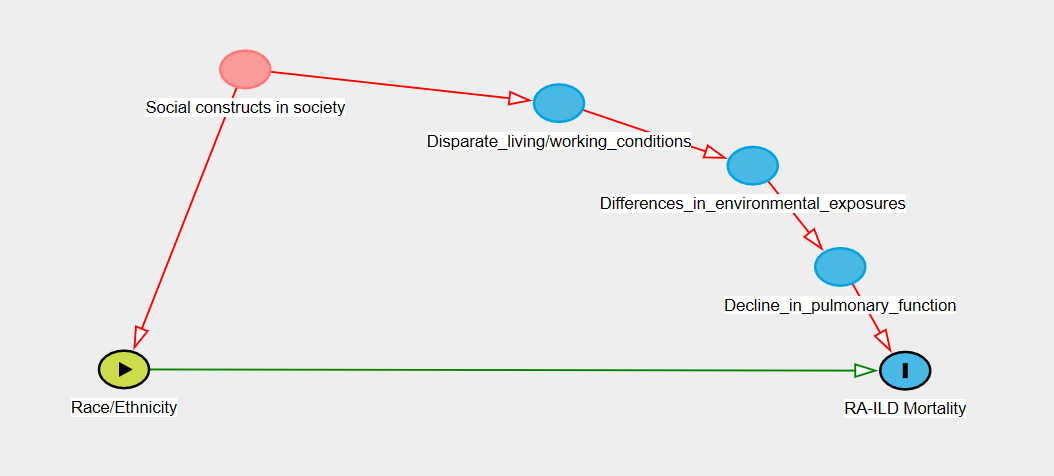
Social constructs are associated with both race and ethnicity (directly) and mortality in RA-ILD through disparate living and working conditions, which leads to environmental exposures that can cause inflammation or scarring in the lungs, which leads to a decline in pulmonary function, which in turn is known to increase mortality in patients with RA-ILD.
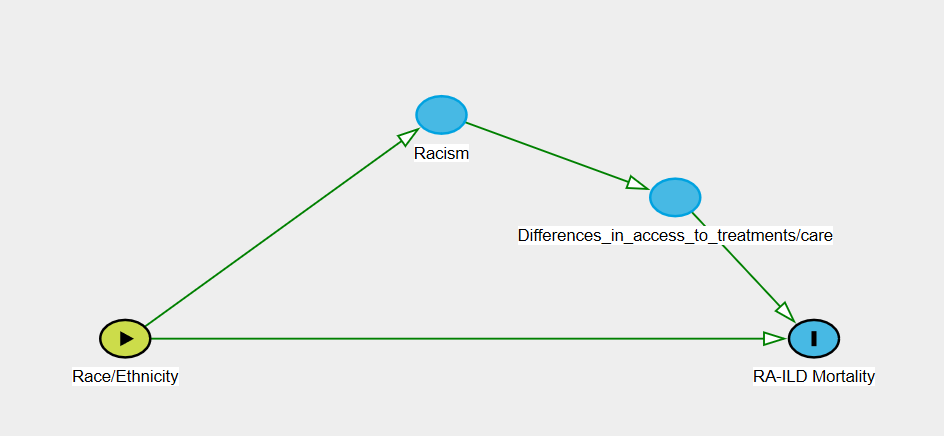
SES as a mediator:
Racism acts as a mediator between a predictor variable of race/ethnicity and an outcome of mortality in RA-ILD through differences in access to care, medications, live saving treatments, etc.
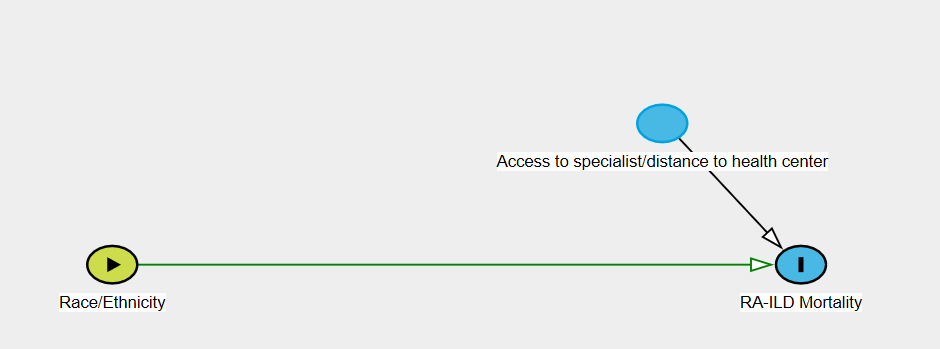
SES as an effect modifier:
Distance to a health center with specialty care would be an effect modifier between race/ethnicity and mortality in RA-ILD via possible delays in diagnosis which could lead to more severe disease at presentation and higher mortality.
2. Describe a potential effect modifier, mediator, or contextual variable (for definition of contextual variable, see Diez-Roux reading) for an association of interest to you and relevant to health disparities. For example, for investigating the association between education and hypertension, I might be interested in evaluating whether the association between years of education and hypertension is different for Black men than for White men. Describe how you would study whether this relationship exists.
I am interested in looking at outcomes in idiopathic pulmonary fibrosis (IPF) (specifically changes in PFTs over time, mortality, and lung transplantation) by rural or urban geographic location. One possible effect modifier to evaluate in this study would be smoking, as this is known to increase risk for IPF, but would not be associated with rural or urban geography. A potential mediator in this analysis would be distance to clinic, as differences in outcomes may be mechanistically related to geography by the amount of time it takes to travel to a tertiary care clinic. Lastly, a potential contextual variable in this case would be median household income, obtained by census tract level from the American Community Survey. This is group level data, as implied by a contextual variable, applied to individual outcomes in our cohort of IPF patients.
I plan to study these associations using multivariate linear regression for the continuous outcomes and logistic regression for those that are binary (death and transplantation). To account for effect modification, I will create an interaction term. To account for mediation, I will create several different models accounting for the relationship between the mediator and the exposure and outcome.
3. Respond to one other person's post on the forum with a comment or suggestion.
Please see Aksharananda Rambachan’s post.