Article: Akinyemiju T, Moore JX, Pisu M. Mediating effects of
cancer risk factors on the association between race and cancer incidence:
analysis of the NIH-AARP Diet and Health Study. Annals of Epidemiology.
2018;28(1):33-40.e2. doi:10.1016/j.annepidem.2017.11.003
What is the primary discipline of the authors? Cancer research, racial disparities- authors are affiliated to a
comprehensive cancer center and departments/divisions of epidemiology, surgery and
preventive medicine.
What is the exposure of interest? The exposure of interest is race (black/African
American or white), self-reported at study baseline.
What is the outcome of interest? Cancer risk. Incident cases
information was linked from cancer registries. Authors evaluated racial disparities
in the risk of any type of cancer and breast, prostate and colorectal cancers
separately. Mediation analyses were conducted for these three types of cancer only.
What is the hypothesized mediator of interest and how is it
measured? The mediators of interest are cancer
risk factors: BMI, smoking status, physical activity, nutrition and alcohol use.
All of them were measured by self-report at baseline using questionnaires and
defined as: BMI (continuous, kg/m2, per SD increase); smoking status
(binary, current vs past/never smoking); physical activity (binary, greater
than or equal to 3 times/week that caused increased breathing, heart rate or sweat);
nutrition (continuous, number of fruit and vegetables servings/day, per SD
increase); alcohol use (binary, less than or equal to 7 alcoholic drinks/week
for women or less than or equal to 14 alcoholic drinks/week for men).
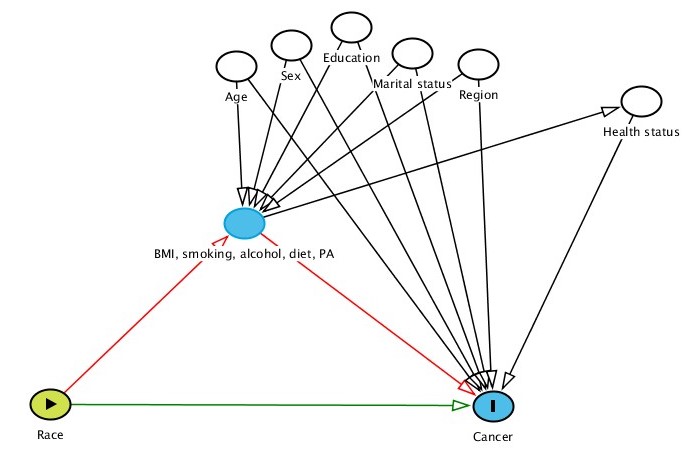
Describe the modeling approach and briefly report the estimated
total, direct, and indirect effects (if these are reported). Authors used the counterfactual approach
to mediation analysis (with survival data) proposed by Valeri and VanderWeele, as
this method allows to decompose the total effect into indirect and direct effects
while accounting for exposure-mediator interactions, nonlinearity and
confounding (exposure-outcome, mediator-outcome, exposure-mediator). In the analysis
authors conducted Cox proportional hazards models (outcome: incident cancers,
exposure: race) which were adjusted for age, sex, marital status, education, health
status and region. Results were reported as hazard ratios and 95% CIs (for natural
direct effects, natural indirect effects and total effects) and proportions
mediated.
Effects, HR (95% CI)
Race and breast cancer
Total
BMI: 0.82 (0.75, 0.90)
Current smoker: 0.83 (0.76, 0.91)
Physical activity: 0.83 (0.76, 0.91)
Alcohol use: 0.83 (0.76, 0.91)
Nutrition: 0.83 (0.76, 0.91)
Direct
BMI: 0.81 (0.74, 0.89)
Current smoker: 0.83 (0.76, 0.91)
Physical activity: 0.83 (0.76, 0.91)
Alcohol use: 0.83 (0.76, 0.91)
Nutrition: 0.84 (0.77, 0.92)
Indirect
BMI: 1.01 (1.01, 1.02)
Current smoker: 1.00 (1.00, 1.00)
Physical activity: 0.998 (0.997, 0.999)
Alcohol use: 1.00 (1.00, 1.00)
Nutrition: 0.988 (0.979, 0.996)
Race and prostate cancer
Total
BMI: 1.84 (1.74, 1.95)
Current smoker: 1.87 (1.77, 1.98)
Physical activity: 1.87 (1.76, 1.98)
Alcohol use: 1.87 (1.76, 1.98)
Nutrition: 1.86 (1.76, 1.97)
Direct
BMI: 1.88 (1.78, 1.99)
Current smoker: 1.87 (1.77, 1.98)
Physical activity: 1.87 (1.76, 1.98)
Alcohol use: 1.87 (1.76, 1.98)
Nutrition: 1.88 (1.77, 1.99)
Indirect
BMI: 0.979 (0.975, 0.984)
Current smoker: 1.00 (1.00, 1.00)
Physical activity: 1.00 (0.99, 1.00)
Alcohol use: 1.00 (0.99, 1.00)
Nutrition: 0.99 (0.987, 0.997)
Race and colorectal cancer
Total
BMI: 1.14 (1.02, 1.26)
Current smoker: 1.14 (1.02, 1.26)
Physical activity: 1.15 (1.03, 1.28)
Alcohol use: 1.14 (1.02, 1.26)
Nutrition: 1.14 (1.02, 1.26)
Direct
BMI: 1.11 (1.00, 1.24)
Current smoker: 1.14 (1.02, 1.26)
Physical activity: 1.15 (1.03, 1.28)
Alcohol use: 1.14 (1.02, 1.26)
Nutrition: 1.15 (1.04, 1.28)
Indirect
BMI: 1.022 (1.017, 1.027)
Current smoker: 0.99 (0.99, 1.00)
Physical activity: 1.00 (0.99, 1.01)
Alcohol use: 1.00 (0.99, 1.00)
Nutrition: 0.98 (0.97, 0.99)
If the direct effect is reported, would you describe this as a natural
direct effect, a controlled direct effect, or something else? As per authors description in the methods these are natural
direct effects, but I do not understand the distinction with the controlled
effect, or what could be something else.
Do you think there is potential measurement error in the mediator
and how would that affect the results? In this study there is potential for measurement error of the
mediators. Due the nature of the data and how it was collected, it is likely
that participants under-report (BMI, smoking status, alcohol consumption) or over-report
(physical activity, nutrition) information. Measurement error can be present in
all five variables and if the scenario I described is true the associations
between mediators and outcome should be stronger. I have a question here; in
order to say the results would be different, is it needed that the measurement
error is differential according to race? I do not think that there would be “differential
misclassification of mediators” by race per se, but perhaps by other factors, such as
education. And what if race influences education? One of the assumptions authors
mentioned for this type of analysis is that exposure does not affect any of the
mediator-outcome confounders. Could race -through enclaves, parental income, people
can’t afford going to better schools out of the neighborhood, etc.- influence education
and then education the mediators? Maybe in this study this is not important
because all participants (members of AARP) probably have similar
characteristics, but could this be a problem in another setting?
Do you think there are unmeasured confounders of the
mediator-outcome association and how would that affect the results of the
mediation analysis? I cannot think of any other unmeasured
confounder, only causes for cancer (genetic, radiation) but not for mediators.
Do you have any critiques of the paper? In general, I think it is a good paper. However, after drawing
the DAG I have a concern about one of the variables they included in the
analysis (so I think was considered as confounder): health status. Authors did
not describe clearly what this variable refers to. For me it is not a cause of
the mediators but an effect of them. Although I was not sure I should, I
included health status as cause of the outcome (also for 5 seconds I thought it
was an effect of outcome and then a collider, but realized it was measured at
baseline when participants were cancer-free; all participants with cancer at entry were excluded). If this is true, there is a
portion of the “ indirect and total effects” that was not captured in the analysis (that additional
path was blocked).