Hi, and thank you for reading my protocol. I attached previous assignments below (green) in case you would like to reference them.
PROTOCOL 4: ORGANZATIONAL CHANGE
1. Describe the organizational and/or delivery system environment in which your intervention will take place.
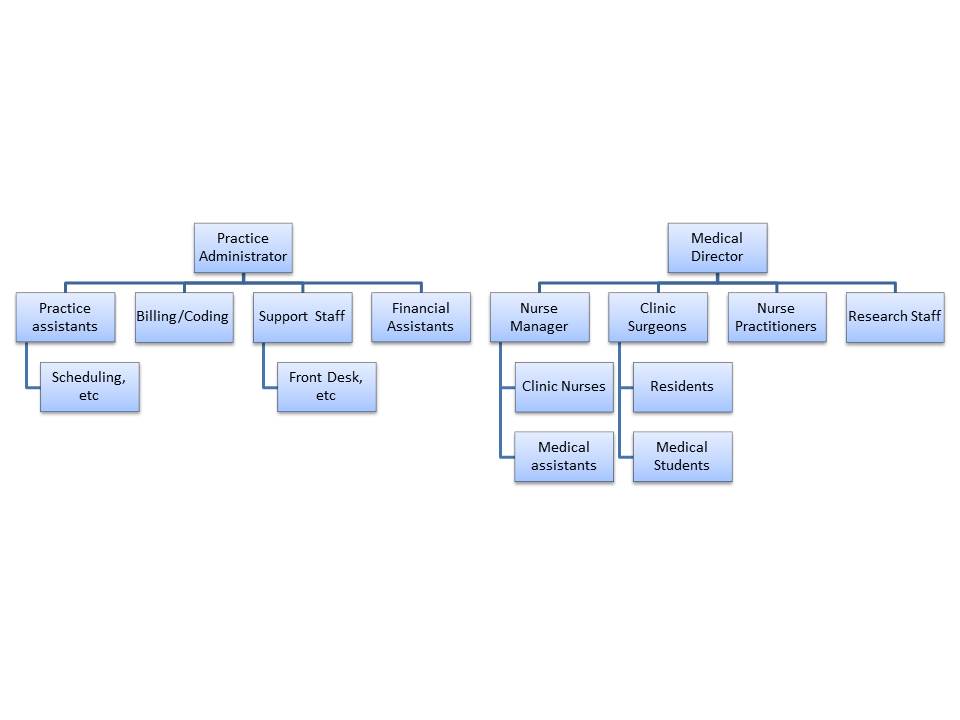
The main organizational environment I will be targeting with my intervention is the general surgery clinic at UCSF. I would eventually like to see it spread to other clinics both within and outside UCSF after we have established a successful model (realizing of course that each site will need an individualized approach).
I will need to do further investigation of the hierarchies involved within the clinic (and I have meetings set up to do this), but my best understanding presently is attached as a figure at the very bottom of the document:
2. Based on Shortell’s 4 domains of organizational change, identify organizational barriers that could potentially impede successful implementation of your proposed intervention.
The main barrier I will face is culture (both among physicians and practice assistants). Current culture among clinic surgeons and residents is varying regarding use of shared decision making. Even in those who accept it as valuable, it is not built into daily surgical practice. Further, this would need to be built into the culture at the administrators side as well because they would be giving the decision aids to patients for use prior to meeting with the surgeon. This adds work that they will not necessarily see the direct results of.
3. Using the same 4 domain model, describe how your intervention plan can take advantage of organizational strengths OR propose practical methods for addressing these barriers within your program.
The most effective way to address the culture barrier will be to engage physicians and practice assistants during the implementation design process with two goals: 1) Everyone is educated about what shared decision making is and why it is important and 2) It is implemented in a way that is consistent with current practice and does not cause undue burden on anyone.
Further, I will plan to continually evaluate and change the implementation strategy as necessary through continuous monitoring of decision aids and shared decision making and feedback of the results to the clinicians and administrators. I will plan to evaluate this on a regular basis so that I know what is and is not working and changes can be made as necessary after engaging the clinic staff.
PROTOCOL 1: INTRODUCTION
Protocol Title: Implementation of Shared Decision Making in General Surgery.
- 1. What evidence are you proposing to translate into practice?
The integration of shared decision making (SDM) during the care of general surgery patients at UCSF. SDM builds on the typical informed consent discussions in surgery by incorporating evidence-based information and patient preferences into decision making. Certain decisions made in general surgery clinics are important targets for shared decision making because the decisions are high risk, preference-sensitive, and more than one option is supported by the evidence. In order to participate in SDM, patients need (1):
- Encouragement by their provider
- Be aware that there is a choice
- Adequate knowledge
- Understand their responsibility and right to participate in decision making
- Have the time to participate
Decision aids are tools used to promote SDM by providing evidence-based education and values clarification exercises. Decision aids have been shown to be effective in improving patient knowledge and participation in decision making in many different clinical scenarios, both medical and surgical (2).
Implementing SDM in general surgery clinics would require at least two major behavioral changes:
- Surgeons would modify informed consent discussions to reflect a SDM framework (and address #1 and #2 above).
- Patients would use decision aids to prepare for the discussion with the surgeon (to address #3-5 above).
- a. Justify that this evidence is “ready for translation.”
A 2014 Cochrane review of decision aids (which included 14 randomized controlled trials of surgical decision aids) found decision aids resulted in increased knowledge, participation in decision making, and clarity regarding personal values while reducing decisional conflict (2). A 2013 meta-analysis of decision aids used in surgical patients had similar results (3). One challenge to synthesizing this data is the sheer heterogeneity of the decision aid tools themselves and the populations they are used in. Overall, these studies show that decision aids are a beneficial adjunct to the patient-physician encounter for a broad range of surgical patient, including those with breast cancer, low back pain, menorrhagia, prostate cancer, abdominal aortic aneurysm, and those considering bariatric surgery.
- b. Identify a single, key behavior change target for your translational activity.
Physician-led shared decision making (for appropriate decisions) in the general surgery clinic (to be bolstered through the use of patient decision aids).
- c. Conduct a “gap analysis” of your target behavior. Look to diverse sources for “best guess” estimates if specific measures are not available.
General surgery patients have not been studied in aggregate, although there is evidence that patients want to be more informed and involved in the decision making process. For example, although 64% of women with early stage breast cancer desire participation in shared decision making, only 33% feel that they had an active role (4). Decision aids are a tool that can be used to promote participation in shared decision making and close this gap.
- 2. What is the quality (performance) gap?
Implementation of decision aids and shared decision making is not widespread and there are no national studies that have looked at their routine use in clinical practice. Indications of the need for increased shared decision making include poor patient knowledge about common medical decisions (5), marked variation in care for preference-sensitive medical decisions (6), and general lack of shared decision making in clinical encounters (7).
- 3. What is the outcome gap?
- Patient knowledge: a meta-analysis of studies measuring patient knowledge after using decision aids for breast cancer surgery showed that patient knowledge increased by 24% following use of the decision aid (8). This was particularly marked in patients with low levels of knowledge prior to using the decision aid. A randomized controlled trial of the decision aid we propose to implement increased knowledge significantly among those assigned to the decision aid compared to controls using a validated knowledge tool (9).
- Patient satisfaction: A systematic review of decision aids used in this patient population showed that patients who were assigned to the decision aid were more likely to report satisfaction with their decision (8).
- Participation in decision making: A meta-analysis showed that decision aids reduced patient’s perceptions of being passive in decision making (RR 0.61 CI .49-.77)
- 4. Is there evidence that changing performance will improve health (clinical outcomes)?
- Patient knowledge: Patients with poor health literacy are more likely to rate their health as poor and use more emergency care than patients with good health literacy (10, 11). This may indicate that patients who are more knowledgeable about their health use less healthcare resources.
- Patient satisfaction: Patient satisfaction is being used as a quality indicator and as a basis for physician reimbursement. Although the impact of decision aids on HCAHPS for patients undergoing surgery for early stage breast cancer is not known, decision aids have been linked to increased patient satisfaction (8).
- Participation in decision making: When patients are actively engaged in their medical care, treatment adherence may increase (12, 13).
PROTOCOL 2 COMMUNITY ENGAGEMENT
- 1. Define the communit(ies) for your project and explain why each is a stakeholder for your study.
Many groups will be important for the implementation of shared decision making in general surgery patients. Without the full participation of any of these groups the project will be essentially impossible. Specifically:
- The patients and their families. Even if I were able to get all other necessary parts of implementation running smoothly, if patients are not interested or engaged, the program will fail.
- Insurance companies – If I were able to get insurance companies interested, there would be the potential to provide physician and patient incentives for using the decision aid.
- Hospital administration/IT – Important for creating a culture of change around this topic. Will need their support for data monitoring as well.
- Clinic Administration – Needed for implementation of decision aids and allowing full implementation of shared decision making.
- Nurses – To be the front line in terms of pitching the idea to patients, providing information about the decision aid, and encouraging patients to use it.
- Physicians – The decision aid is part of promoting a culture of shared decision making. In order for shared decision making to work, it requires full patient and physician participation.
- 2. Describe your plan for approaching potential community partners to ask for their involvement.
- Patients and families: I would consider using the patient advisory council to get feedback on the protocol and the decision aid. Patients would need to be actively engaged before appointments by nursing staff. It would be ideal to have a computer in clinic that patients could use to view the decision aid. This will be particularly important for those with limited computer access.
- Insurance companies: I could share the information that the affordable care act contains language that could ultimately result in linking payments to the use of decision aids. In addition, I can show evidence that decision aids result in higher patient satisfaction and reduced costs (not this aid in particular, but there are several aids that do).
- Hospital administration: Would work more from the patient satisfaction standpoint, because reimbursement is linked to patient satisfaction scores. I would also plan to give the administration monthly reports of outcomes and implementation data so they can participate in re-iterating the protocol and can help reinforce positive behaviors in staff.
- Clinic Administration/IT: Would need to provide education about SDM – why it is important and determine how it can be integrated into the current system of care.
- Nurses/physicians: would start by reaching out to them, understanding the current patient education interventions and patient flow, and determining which decision aids might be most acceptable and appropriate from their point of view. Would really emphasize that this is meant to improve clinical care for patients. Would try to gauge what outcomes would be meaningful and relevant from their perspective.
- 3. Identify which stages of your project you'll incorporate community input, and describe what types of input you'll solicit.
- The first group I would get feedback from would be physicians and nurses. I would have them view the aid and work with them to develop an appropriate process for implementing it. Once that was completed, I would present the protocol to patients (perhaps through the patient advisory council or focus groups) to determine what the interests and barriers are in that population. I would then move to the clinic administration and IT groups to determine how we could best implement it within the current clinic structure. The last group I would go to would be hospital administrators and insurance companies.
- 4. Name three ways you plan to share your results, beyond writing an academic article or presenting at an academic conference.
- Monthly feedback of data to administration and individual physicians (full transparency)
- Write an article for the lay press
- Write an article for the UCSF website
PROTOCOL 3: THEORIES OF IMPLEMENTATION
- 1. Identify a patient or community group that contributes to or is involved in the principal behavior you are attempting to improve with your intervention.
I think that surgeons would be the primary target of this intervention. Although it takes patient engagement, which I propose facilitating through the use of decision aids, ultimately, the surgeon must lead the shared decision making process during the appointment in clinic.
- 2. Using any of the individual explanatory theories in “Theory at a Glance”, develop an explanatory model for the target behavior (above) that you will be attempting to influence with your intervention.
Please see figure. All data derived from the expected results of discussions with surgeons regarding their beliefs, expectations, and experiences with shared decision making. White boxes indicate theory, blue boxes indicate interventions.
- 3. Identify how one or more of your specific interventions will target one or more of these key factors contributing to the behavior of interest.
Please see blue boxes: interventions will include the implemention of patient decision aids, surgeon education, and timely feedback to surgeons during the implementation process.
- 4. Create a framework that draws upon a socio-ecological framework to orient your target behavior within a larger context.
- Social and Economic Policies: Because social, economic, and health policy are so dependent on each other this will be a long-term and important component of the wide spread adoption and implementation of shared decision making. Already, it is mentioned in the Affordable Care Act, and several states are beginning to implement legislation that could tie shared decision making to physician reimbursement (14). As evidence accumulates about the effectiveness of shared decision making and the implementation process, I think it will become even more widespread.
- Institutions: Will be responsible for facilitating and inspiring physicians to use shared decision making. Most likely in response to social, economic, and health policy.
- Neighborhoods and Communities, Living Conditions, and Social Relationships: Without patient buy-in, shared decision making will never work. One key component is that patients desire to participate in and take responsibility for their health care. This can only occur by empowering communities and ensuring access to other, more basic human needs (healthy food, housing, employment, etc).
- Individual and Population Health: Health has a complex relationship with community factors, living conditions, and social relationships, and improving health through shared decision making could have an important impact on improving these other factors.
1. Fraenkel L, McGraw S. What are the essential elements to enable patient participation in medical decision making? Journal of general internal medicine. 2007;22(5):614-9.
2. Stacey D, Legare F, Col NF, Bennett CL, Barry MJ, Eden KB, et al. Decision aids for people facing health treatment or screening decisions. The Cochrane database of systematic reviews. 2014;1:Cd001431.
3. Knops AM, Legemate DA, Goossens A, Bossuyt PM, Ubbink DT. Decision aids for patients facing a surgical treatment decision: a systematic review and meta-analysis. Ann Surg. 2013;257(5):860-6.
4. Keating NL, Guadagnoli E, Landrum MB, Borbas C, Weeks JC. Treatment decision making in early-stage breast cancer: should surgeons match patients' desired level of involvement? Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2002;20(6):1473-9.
5. Fagerlin A, Sepucha KR, Couper MP, Levin CA, Singer E, Zikmund-Fisher BJ. Patients’ Knowledge about 9 Common Health Conditions: The DECISIONS Survey. Medical Decision Making. 2010;30(5 suppl):35S-52S.
6. O'Connor AM, Llewellyn-Thomas HA, Flood AB. Modifying unwarranted variations in health care: shared decision making using patient decision aids. HEALTH AFFAIRS-MILLWOOD VA THEN BETHESDA MA-. 2004;23:VAR-63.
7. Braddock CH, 3rd, Edwards KA, Hasenberg NM, Laidley TL, Levinson W. Informed decision making in outpatient practice: time to get back to basics. JAMA : the journal of the American Medical Association. 1999;282(24):2313-20.
8. Waljee JF, Rogers MA, Alderman AK. Decision aids and breast cancer: do they influence choice for surgery and knowledge of treatment options? Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2007;25(9):1067-73.
9. Jibaja-Weiss ML, Volk RJ, Granchi TS, Neff NE, Robinson EK, Spann SJ, et al. Entertainment education for breast cancer surgery decisions: a randomized trial among patients with low health literacy. Patient education and counseling. 2011;84(1):41-8.
10. Baker DW, Parker RM, Williams MV, Clark WS, Nurss J. The relationship of patient reading ability to self-reported health and use of health services. American journal of public health. 1997;87(6):1027-30.
11. Baker DW, Gazmararian JA, Williams MV, Scott T, Parker RM, Green D, et al. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. American journal of public health. 2002;92(8):1278-83.
12. Vermeire E, Hearnshaw H, Van Royen P, Denekens J. Patient adherence to treatment: three decades of research. A comprehensive review. J Clin Pharm Ther. 2001;26(5):331-42.
13. Robinson JH, Callister LC, Berry JA, Dearing KA. Patient-centered care and adherence: definitions and applications to improve outcomes. Journal of the American Academy of Nurse Practitioners. 2008;20(12):600-7.
14. Frosch DL, Moulton BW, Wexler RM, Holmes-Rovner M, Volk RJ, Levin CA. Shared decision making in the United States: policy and implementation activity on multiple fronts. Zeitschrift fur Evidenz, Fortbildung und Qualitat im Gesundheitswesen. 2011;105(4):305-12.