Protocol #1: Quality & Outcomes Gaps
A. What evidence are you proposing to translate into practice?
I am proposing to translate evidence on the benefits of continuous labor support (physical, emotional and informational) on labor and delivery outcomes, for both mother and infant, into practice.
A1. Justify that this evidence is “ready for translation.
A Cochrane Systematic Review was updated and released in July of 2013 summarizing results of 22 randomized controlled trials with data from 15,288 women. These review found strong results of the many benefits of continuous labor support, including reduced likelihood of cesarean section, lower likelihood of using analgesia, lower likelihood of patient dissatisfaction, shorter labors, and lower likelihood of instrumental vaginal birth. Subgroup analyses suggest that continuous support is most effective when the provider is not part of the woman's social network.
A2. Identify a single, key behavior change target for your translational activity. The single, key behavior change target for my translational activity would be to get hospitals in San Francisco to routinely offer doula services to their clients - ideally, to introduce them in the prenatal period, but if not, to offer when woman arrives in labor (modeled after SFGH program).
A3. Conduct a “gap analysis” of your target behavior. Look to diverse sources for “best guess” estimates if specific measures are not available.
To the best of my knowledge, SFGH is the only hospital in SF that offers doula services to all patients. Several other hospitals will allow a woman to have a doula present, but do not facilitate these services and are at times resistant to them.
B. What is the quality (performance) gap?
Per above, the performance gap is that only one hospital in the Bay Area routinely offers doula services to all patients - regardless of ability to pay. There are many other hospitals in the area that could be providing these services.
C. What is the outcome gap?
The outcome gap is that right now, roughly 30% of women deliver via cesarean section. The WHO and numerous other organizations feel that the maximum proportion of births ending in c-section should be 15%, and generally closer to 5-10%. Doula continuous labor support has been shown to dramatically reduce the rate of cesarean sections - by up to half - and this could result in much improved outcomes for both the mother and child, as well as an enormous reduction in hospital costs/expenses.
D. Is there evidence that changing performance will improve health (clinical outcomes)? Yes, there is strong evidence that changing performance would improve outcomes. Again, the Cochrane review cites 22 RCTs looking at this question, consistently showing the benefit of continuous labor support.
Protocol #2: Community Engagement
1. Define the communit(ies) for your project and explain why each is a stakeholder for your study.
The key communities involved in my project will include the following groups, at the hospital(s) within which I end up trying to implement this project:
- Hospital Administrators: These individuals will be crucial to engage because they will be the ultimate "decider" as to what will be allowed to be implemented in the hospital and what will not. They will have the greatest understanding of what the administrative, legal and financial barriers might be, and how they might be overcome.
- Payers/insurance companies: Identifying how labor and delivery services are reimbursed to hospitals, and how reductions in c-sections may change payment to hospitals. Also, whether or not payers would be willing to reimburse CLS/doula services directly for patients.
- All labor and delivery personnel (physicians, midwives, nurses, other): These individuals are currently the team that provides all labor and delivery care to women within the hospital. The introduction of CLS/doula services would a fairly significant intervention, and the current team of providers at the hospital would need to be willing participants for any intervention to work. Education of these providers regarding the documented benefits for women and infants of CLS will be crucial to securing provider buy-in and engagement. Careful explanation of how it will and will not change things will also help.
- Prenatal care clinic personnel: These individuals can be engaged to let them know about the intervention planning process, what forms it may take, and how they could be involved in terms of informing their patients.
- Neonatologists and pediatricians: These individuals could also be engaged about the design and purpose of the intervention, and hopefully to secure their buy-in based on the documented benefits to infants from CLS.
- Pregnant women seeking prenatal care: Eventually, these women will be the "end-users" of the intervention. They will be the ones to directly benefit, physically and emotionally, from the CLS intervention. During the design phase, these women could be consulted for what they would want in an ideal intervention, what there concerns are, etc. After implementation, these women would be educated about the existence of the program, and also consulted on their satisfaction with it and room for improvement (evaluation).
- Implementers of Doula program at SFGH: There is one permanent/in-house CLS/doula program at SFGH. The midwives who started this program are an invaluable resource in terms of their accumulated experience/wisdom in how to go about implementing and establishing a similar program elsewhere. They will be crucial in the very initial planning stages to understand what should be done, when, and how.
- Add Doulas!
2. Describe your plan for approaching potential community partners to ask for their involvement.
My plan for approaching potential community partners for their involvement varies for each partner, as detailed below. I feel that the order in which I reach out to these various communities is very important as well. I would want to have had several thorough conversations with a number of community members before reaching out to the more high-level, sensitive, communities - such as Hospital Administrators. I've listed the communities in order of which I think I should reach out to them. Question: Is there any particular literature on how to strategize the ordering of your communication with various levels/subsets of your targeted communities?
- Implementers of Doula program at SFGH: I personally know the founders and organizers of the SFGH Doula program and can reach out to them directly, once I've gotten a bit more organized.
- Payers/insurance companies: I would love guidance on how to be more strategic/systematic on this piece - but my initial thought is that I could simply contact several major insurance providers for SF hospitals and ask them how they reimburse for different L&D services. This sort of contact information is usually available publicly on their websites. Alternatively, I could call the L&D departments at several SF hospitals and ask for a direct line (if any) to the insurance companies that they routinely deal with. Any advice?
- Labor and delivery personnel (physicians, midwives, nurses, other): Thankfully, Dr. Gonzalez has put me in touch with Dr. Sawaya, who has given me the phone and email contact of several senior people within UCSF's L&D departments - both at SFGH and UCSF. These individuals will be a great first point of contact in these departments (I think), and from there, could refer me to others that I could speak with. As the intervention design develops, I would eventually want to work with/through these L&D leaders to help hold sessions with L&D personnel to describe why we think this intervention is needed, their reactions to it, concerns, questions, logistics, etc.
- Pregnant women seeking prenatal care: Again, as the intervention design moves further along, perhaps women seeking prenatal care could be offered the option of filling out a survey about their thoughts/reactions on CLS services while waiting for their appointment.
- Hospital Administrators: Only after I've gathered much more information about the nuts and bolts of what this intervention could look like, the cost-savings it might have (specific to SF payer systems), and have initial buy-in from L&D personnel (at least at the senior level), I would ask for an introduction to hospital administrators from someone with a direct connection - ideally someone that I have been working with from L&D or UCSF regarding this project.
- Prenatal care clinic personnel, neonatologists and pediatricians: For this community, I would ask to be introduced to leaders within each hospital for these departments and would email them to set up a time to discuss the idea, what it might mean for them, gather their thoughts, answer any questions, etc etc. I think this could come later for this group, as they would not be as directly effected.
3. Identify which stages of your project you'll incorporate community input, and describe what types of input you'll solicit.
In terms of which stages of my project I will incorporate the community input from the above stakeholders, I tried to outline that above. In the very early stages, I will want to incorporate community input from the founders of the SFGH doula program, senior members of the Labor & Delivery unit teams, and the insurance companies. Explicitly creating a stakeholder advisory group comprised of these individuals may be helpful in terms of formalizing their involvement, and generating richer feedback with the combined experiences of all groups. I would then take the information gathered from these initial data gathering conversations, and approach Hospital Administrators to gain a better understanding for what information they need and want to see in order to be convinced that it is a good idea for their hospital. Then, I would return to my initial stakeholder advisors to solicit further input. If we are able to proceed to intervention (at least in some small form), I would first work with target hospital staff to organize a forum for talking to the L&D staff (nurses, midwives, physicians and others) about explaining what CLS is, what it would mean day to day, the benefits it has on maternal and infant outcomes. I would then want to build in a lot of opportunities for these individuals to express questions and concerns and suggestions. Once implementation begins, I would want to have ongoing forums and guidelines for data collection, as well as for conversation, feedback, and questions from all L&D staff, as well as from more peripherally involved units, such as prenatal care and postpartum care of mother and infant, and from mothers/patients themselves. After some finite period of time, we would evaluate the data collected thus far on patient outcomes (both maternal and infant), L&D staff experiences/satisfaction, patient satisfaction, costs, and other outcomes identified in conversation and planning with community members.
4. Name three ways you plan to share your results, beyond writing an academic article or presenting at an academic conference.
During the initial three months of implementation, bi-weekly reports will be circulated to L&D staff (including new doulas), documenting how many births occurred, % attended by doulas, differences in c-section rates by doula vs non-doula attended, as well as secondary intervention outcomes such as differences in pain medication use, patient satisfaction, and instrument assisted delivery between doula and non-doula assisted births, as well as documenting concerns and suggestions offered by staff. I would ideally like to hold a regular meeting - perhaps monthly or timed bi-weekly with the reports - for staff to convene in person and voice frustrations, successes, etc.
Secondly, part-way through the intervention (perhaps after 6months? 1 year?), I would aim to gather leaders from other L&D departments and hospital adminstrators from across San Francisco to present the results of our intervention so far, including hard numbers as well as staff and patient subjective experiences. The aim of this meeting would be to introduce the idea to other hospitals, assuming our work has been effective, and encourage them to consider adoption. If the intervention is NOT successful, convening this meaning may help to generate insight into why it was not successful, and if there are possible solutions. Finally, I would also present the findings from the intervention to a larger maternal health care quality improvement collaboration or institute - at the regional or national level - to propose scale and expansion to other hospitals in other areas.
Protocol #3: Mapping
1. Identify a patient or community group that contributes to or is involved in the principal behavior you are attempting to improve with your intervention.
For the purposes of this protocol, I am focusing on the laboring woman (the patient) as the individual to whom I am targeting the behavior change intervention – requesting continuous labor support (via doula services) in a hospital delivery setting.
2. Using any of the individual explanatory theories in “Theory at a Glance”, develop an explanatory model for the target behavior (above) that you will be attempting to influence with your intervention. This can be an extension/based on expected findings (or previously published literature) from your answers to Homework #3. Figures are always very useful... keep it simple.
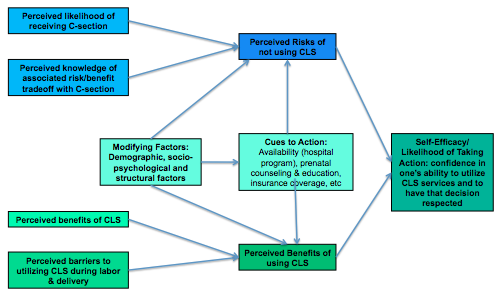
Although slightly simpler, I think that the Health Belief Model may fit the individual/patient centered decision process of my proposed intervention. I believe that most women are not aware of the option of continuous labor support, or of its many benefits. Further, I also think many women aren’t aware of the relative risks of many common labor and delivery interventions, or of how frequently they are employed in the US hospital setting. Thus, successfully getting women to adopt the use of continuous labor support (CLS) during their delivery seems to me to be mostly a matter of promoting awareness/education, and of providing access. See the below model (attached).
3. Identify how one or more of your specific interventions will target one or more of these key factors contributing to the behavior of interest.
One component of my proposed intervention will be an introduction/discussion of CLS during prenatal visits at the hospital with pregnant women. These discussions will introduce what CLS is, describe what it looks like, the benefits and possible risks, and provide women information to reach out to individual doulas, as well as women who have and have not used doula services at this hospital in the past. This intervention will address the both the perceived benefits aspect of the above model, as well as provide a cue to action for the woman.
4. Create a framework that draws upon a socio-ecological framework to orient your target behavior within a larger context. ie, what are some of broader, external forces that influence the individual behavior of interest...see Figure 2 of “Theory at a Glance.”
I think the most important external force that will influence the individual behavior of interest (option for CLS) will be whether or not hospital administration decides to allow a formal CLS program on the L&D ward. However, this influenced is situated within even larger contexts of local, regional, and national health protocols, policies, laws, malpractice climate, insurance/payer influences, and more. I believe that the patient (the laboring woman) is at the core of this proposed intervention, but the patient is embedded in individual and family norms and desired, which is in turn influenced by and centered within local culture and local options (access), which is in turn influenced by local physician training and exposure, which is influenced by hospital policy and protocol, which is itself determined in part by payer systems of reimbursement, legal liability issues, and culture, and so on, and so on.