Reflect on your experience or knowledge regarding use of SGAs in adolescents or youth.
How does this article impact how you monitor adolescents or youth?
Does this article trigger any new questions you have about SGAs in youth?

I would like to start by disclosing, I have no experience in furnishing SGAs in adolescents or youth since I work with adults only. I have definitely furnished
SGA’s for transitional youth ages 18-late 20’s in emergent or urgent psychiatric care.
In urgent care I have been mindful of the SGAs I choose weighing efficacy with metabolic risk while looking at patient’s medication history as well. Often when I see patients they have already tried several anti-psychotics and may have established adverse reactions or side effects to certain SGAs already. Other barriers may be getting insurance coverage for some of the newer SGAs that have a better metabolic risk profile such as Abilify or Lutuda if patient is drug naïve. Many insurance companies want to know that other more affordable medications were tried and proven ineffective or not tolerated well before trying the more expensive medications.
Since I have furnished meds mostly in urgent care settings I have not had the opportunity to monitor individuals weight, BP, lipids and glucose over time to see if the medication is causing metabolic syndrome risk in the patient. As patients repeatedly present to the urgent care clinic I have worked at I have definitely seen their weight wax and wane secondary to SGAs, substance use and life style issues.
Although the Vandenberghe et al. article may have some confounders such as not measuring the patients height with weight over time or factoring in weight gain from additional meds the patient may have been on at the same time of the SGAs, it does make me more cognizant of weight gain potential as early as the first 30 days of treatment.
I believe that detecting and treating psychosis during adolescents and youth is a very key moment that shadows that individual’s trajectory of their illness. It is an extremely vulnerable time. The individual is developing autonomy from parents and are hit with a life changing illness. It is very difficult to get this age group to buy into the importance of treatment. Self-image is important, physical health is important and many of these meds have the side effect of lethargy, mental cloudiness and weight gain. Because of this patients often feel as if the meds are making them sicker instead of controlling an illness that these patients and their families may very well be on the fence of whether there is a mental illness or not. All these factors make it really important to monitor patient’s symptoms, side effects objective and subjective more closely at this age and make changes appropriately in concert with patient and family so that the illness is carefully controlled. This includes factoring in how the patient and family regard the side effects of the meds. If issues are arising that demonstrate metabolic syndrome risk this needs to be discussed carefully weighing the pros and cons of stopping and or changing the medication. I appreciate the Dayabandara et al. article that encourages interventions for metabolic risks instead of ceasing medications that exhibit this risk but demonstrate good control of patient psychotic symptoms. Making patients and family feel that the decisions around risk factors are being made with there input helps these patients continue to stay in treatment and seek treatment in the future. With out including them in these decisions there is potential of alienating them from treatment, which increases the risk of the patient fumbling many times on and off meds. This could repeat many times until the illness has become so debilitating that the patient has lost many of their resources such as housing, care givers and/or developed comorbid illnesses such as substance abuse.
The Vandenberghe et al. and article is hopefully the 1st of many that will study possible ways for treating adolescents with SGAs to develop guidelines for reducing metabolic syndrome risks.
I have attached a meta-analysis study on metabolic syndrome risks with treatment of schizophrenia with anti-psychotics in the adult population. It has helpful guidelines regarding types of antipsychotics and lifestyle issues that factor into these risks, which mirrors the wonderful Dayabandara et al. article Mr Gomez also posted for follow up on our discussion.
Thanks for a great discussion on this important issue.
References
Cooper, S. J. & Reynolds, G. P., (2016). BAP guidelines on the management of weight gain, metabolic disturbances and cardiovascular risk associated with psychosis and antipsychotic drug treatment. Journal of Psychopharmacology. Pg. 1-32. DOI: 10.1177/0269881116645254
Dayabandara, M., Hanwella, R. Ratnatunga, S., Seneviratne, S. Suraweera, C. & A de Silva, V. (2017). Antipsychotic-associated weight gain: management strategies and impact on treatment adherence. Neuropsychiatric Disease and Treatment. 2017:13: 2231-2241.
Vandenberghe, F., Najar-Giroud, A., Holzer, L. Conus, P., Eap C. B., & Ambresin, A. E., (2017). Second-Generation Antipsychotics in Adolescent Psychiatric Patients: metabolic Effects and Impact of a Early Weight Change to Predict Longer Term Weight Gain. Journal of Child and Adolescent Psychopharmacology. 20: 1-8. DOI: 10.1089/cap.2017.0038
I enjoyed discussing the article by Vandenberghe et al. (2017) this week in journal club because it elucidated important factors surrounding second generation antipsychotics and its effects in adolescent patients. What I’ve been enjoying most about journal club is that we get to break down these articles and critically think and reflect on the data that is being presented. Similar to Adrienne, I don’t have any experience prescribe antipsychotics to pediatric or adolescent patients. My only experience has been working with adult and geriatrics in a mental health setting. I felt this article was a good foundation for me in understanding some of the metabolic implications that these medications have with this patient population.
This article impacts how I monitor adolescents and youth in a few different ways but essentially it is similar to how I would monitor adults and geriatrics. We discussed in journal club this week that there is already well-established data that these second-generation antipsychotics are notorious for causing weight gain and metabolic syndrome in patients. This article makes me reflect how serious metabolic syndrome can be in patients and how it can potentially worsen other comorbid conditions. However, with that said, patients that are starting these medications at a younger age are potentially more likely to gain weight for a variety of reasons other than the medications. Due to the variety of ways they gain weight makes me more mindful of worrisome implications surround prescribing and monitoring patients a little more closely. I would monitor labs and weight fluctuations more closely and also provide a lot of psychoeducation to patients and their parents regarding side effects and when to be concerned.
This article triggers a few questions regarding SGAs in pediatric and adolescent patients. I question if a provider may jump to one of the weight neutral medications instead of jumping to some of the well-known offenders like olanzapine. I know every patient will be different because not all patients will respond the same to medications like everyone else. This article did not mention any recommendations that providers can do if patients gain excessive amounts of weight. My understanding is that most providers might discontinue the medication and start something in its place to see if they can target certain symptoms. I do believe that this article will be a good foundation for further research pertaining to SGAs in pediatric and adolescent populations. It will be interesting to see if there will be more recommendations regarding these medications and what we can do as providers to help prevent weight gain that leads to metabolic syndrome.
Hi Adrienne,
I appreciate your experience in working in the acute setting and the reminder of how important it is ensure that a medication can provide good control of psychiatric symptoms first and foremost. Thanks for the review article for adults too, since that it the population age that I am working with currently.
As you and many others mentioned, weight gain is no small issue for youth/young adults, and even adults who have struggled with weight for much of their lives. It's something that none of us should take lightly (I don't think we do) as a side effect of prescribing SGAs (or mood stabilizers) that can cause weight gain. One of the first interventions that review articles recommend (Cooper & Reynolds, 2016; Dayabandara et. al, 2017) are lifestyle modifications and switching antipsychotics. Right now I am managing an adult patient with newly diagnosed Bipolar disorder. While for now she is willing to continue with her current medications, she is very clear that she is not happy with her weight gain side effects. But she is recently stabilizing, and my concern is that if I switch her medications now, she is at great risk of relapse with very little (or no) time of stability. Also, I'm not even sure if switching her medications will result in less weight loss. In terms of lifestyle modifications, this is something we address with each session, but she is also trying to manage a whole lot of different factors in her life that I am not sure how effective that will be either. It's really challenging to hold this knowledge that the weight gain may one day cause her to stop her medications, but at the same time not wanting to make medication changes because the benefits currently do not outweigh the risks. One thing I am falling back upon is the "common factors" of my interactions with her-- being empathetic and understanding of her situation. I am acknowledging the adverse side effects, asking her what her motivations are for continuing with medication, and explaining my rationale for wanting her to stick with the current medication regimen. I really like Shea's (2006) tips that emphasize doing the best we can to have patients make the decision to stop or take medications with us instead of on their own. Patients will decide if medications are worth the side effects, but if they make that decision with us, at least we can have our input in the decision.
Cooper, S. J. & Reynolds, G. P., (2016). BAP guidelines on the management of weight gain, metabolic disturbances and cardiovascular risk associated with psychosis and antipsychotic drug treatment. Journal of Psychopharmacology, 30(8): 717-748. doi: 10.1177/0269881116645254
Dayabandara, M., Hanwella, R., Ratnatunga, S., Seneviratne, S., Suraweera, C., & de Silva, V. A., (2017). Antipsychotic-associated weight gain: management strategies and impact on treatment adherence. Neuropsychiatric Disease and Treatment, 13, 2231-2241.
Shea, S. C., (2006). Improving medication adherence: How to talk to patients about their medications. Philadelphia: Lippincott Williams & Wilkins.
Hello everyone, I really enjoyed the presentation by Seth and the points of interest that were brought to light. Like many of my peers, I have little to no experience prescribing SCA’s to youth. This is not my area of practice; however, the article was quite moving and the discussion that followed was even more interesting. Seth encouraged us to google the authors name to see if this subject was really their area of passion. I never thought of doing that before or after reading an article written by an author. There were several points brought to my attention during the presentation that caused me to stop and take note. Some were common knowledge and some really surprised me. My top five were :1) SGA’s cause the most weight gain especially in youth. 2)At which point should the caregiver start to intervene once the medication has begun and the youth is noticeable gaining a significant amount of weight.3) This article, though it is the first of its type to include youth, should serve as an agent to develop guidelines in the administration of SGA’s and the perpetual weight gain acquired by youth. 4) Care givers should be educated about weight gain among youth receiving SGA’s. and 5) Weight gain in the youth appears more dramatic than weight gain in an adult due to the development and transition that their bodies are experiencing. Many other ideas were brought to light as well, for instance, the article did not mention other medications that could also contribute to some of the weight gain acquired by the youth. Retrospective studies are less labor intensive because material used in them is already gathered.
I really enjoyed the contribution expressed by my peers in the discussion. It was amazing that everyone was familiar with most of the SGA’s except one (amisulpride). The reason was it is not available in the US market yet. The general consensus of the group was that more research needed to be done before the medical community could take a firm stand on the final conclusion reached by the authors. I really enjoyed the discussion and look forward to our next gathering.
Although I hope to work with youth as a nurse practitioner, I have limited experience prescribing SGAs to youth/adolescents at this point in my training, and even less experience monitoring/preventing weight gain. At my clinical site most of the children that we see are being treated for anxiety, depression or ADHD, so SGA's are rarely used. We worry most about weight loss/failure to gain weight for clients who are taking stimulants, and rarely have to focus on preventing weight gain for individuals on antipsychotics. That said, my preceptor and I have started a few adolescents on Risperdal, Seroquel and Abilify for psychosis or in one case for mania.
Despite the fact that the population in this study is not very reflective of the children/adolescents I see (for reasons discussed in the Journal Club session), this article has served as a good reminder to me about the importance of monitoring weight gain in youth on SGAs. Because we don't see many youth taking these medications at my clinical site, I do not have much experience seeing individual clients gain large amounts of weight. This may be due to the fact that I am new at functioning as a provider, but I suspect it may be more due to a lack of awareness and a tendency to minimize small amounts of weight gain. This article serves as a good reminder, though, of the importance of monitoring weight in youth taking these medications because of the associated risk with later obesity and metabolic syndrome.
Something I found to be particularly interesting is the idea that even a very small amount of weight gain can be predictive of later problems. This drives home the importance for me of closely monitoring weight, talking about the risks of weight gain with kids/parents and employing tactics to prevent weight gain before it happens.
In the article and class discussion, we discussed how SGAs are often more problematic in younger patients because they are more sensitive and susceptible to weight gain due to changes in puberty and hormonal changes. Additionally, teens may not have yet established healthy habits that are necessary for weight loss/weight maintenance such as regular exercise and eating a balanced, healthy diet. After reading the article and discussing it amongst the group, the take away is that substantial and rapid weight gain in the first month of a SGA in an adolescent might be predictive of continual weight gain in the future. I also think that this article might be useful in providing evidence to insurance companies or the court in the context of JV-220s to get approval for more weight-neutral SGAs before trialing several other SGAs that have higher risk for metabolic syndrome. For example, one teen in the group home gained almost 20 lbs over the first few months on quetiapine. It might be useful to print out a copy of this article, and present the evidence that he gained far above the recommended 4% in the first month, and therefore, a more expensive weight-neutral SGA is indicated over trialing a different, more inexpensive SGA such as olanzapine. In future practice, it will helpful to have the 4% parameter as a general rule of thumb to keep in the back of my mind, and to meticulously monitor labs and and intervene early when adolescents have substantial weight gain in the first 1-3 months on an SGA.
I must say that I have limited experience prescribing to adolescents and even less with children in general. My primary group of focus is the adult and geriatric population. It seems to be that there are some similarities in these two populations. As discussed in our journal club this week, second generation antipsychotics (SGAs) are known to cause adverse effects, especially weight gain among other metabolic side effects. When working with the geriatric population is it imperative to start slow and go slow. Not only because this is good practice, but because there are usually many comorbid conditions that can be exacerbated by SGAs. Within the adolescent population it is also important to start low and go slow as their bodies are in a crucial developmental period with hormonal changes that can be effected by introducing SGAs at this phase in life in addition to the known side effects.
As discussed in journal club, I believe that the article just reinforces my monitoring and education practices for all of my clients. It is important to not only be mindful of SGAs adverse reactions and the side effect profiles, but to be continuously monitoring for these effects in all of our clients. The article that we discussed did trigger some questions regarding the long-term effects of SGAs. The article correlated that a >4% weight gain was the likely hood of continued weight gain and complications at later dates (Vandenberghe, et al., 2017). While the data points in question have some holes in them, I do see there is a correlation. Other research has been conducted regarding psychotropic medications and like the Vandergerghe study, they were able to see a correlation with a short-term weight gain with psychotropic medications (Reekie, et al., 2015). But more research is needed to understand the long-term effects of these medications. I would like to know more about these long-term effects and another concern would be how this message is posed to such a vulnerable population that generally have such a focused view on their own body images without being told they will likely gain weight from these medications.
References:
Reekie, J., Hosking, S. P., Prakash, C., Kao, K. T., Juonala, M., & Sabin, M. A. (2015, May 28). The effect of antidepressants and antipsychotics on weight gain in children and adolescents. Obesity Reviews, 16(7), 566-580.
Vandenberghe, F., Najar-Giroud, A., Holzer, L., Conus, P., Eap, C. B., & Ambresin, A.-E. (2017). Second-Generation Antipsychotics in Adolescent Psychiatric Patients: Metabolic Effects and Impact of an Early Weight Change to Predict Longer Term Weight Gain. JOURNAL OF CHILD AND ADOLESCENT PSYCHOPHARMACOLOGY, XX(XX), 1–8.
I have no experience with adolescents or youth that are using or have been prescribed Second-generation antipsychotics (SGAs), however, I just cannot imagine the challenges a child, so young already prescribed medications that not only have some serious side effects, but also affects them in multiple aspects of their lives has to endure. They must deal with stigma, accept this mental health diagnosis at such a young age (which will stay with them for the rest of their lives), and trying to function as a regular kid in the community. Therefore, if we are going to prescribe SGAs to adolescents or youth, we must make sure that we provide them with all the resources and tools to help them work through this diagnosis as simply and easy as we can. And that involves educating, providing of resources, and incorporating other treatment regimens.
I don’t work with adolescents or youth, however, if I were to prescribe or inherit a patient who is taking a SGA, I would make sure to educate them from the beginning, therefore, giving them the knowledge to look out for any side effects that could be developing. I would make sure to have my baseline labs and physical, weights, etc. so that I can compare down the road if there seems to be any new or drastic changes. This article did not really impact how I would monitor, but instead, reminded me that there are parameters to help us monitor, but some parameters are not ideal, therefore, we must trust our own assessments, intuition, and patient’s reports and to tailor each treatment regimen to the individual patient.
If I were a regular person with no knowledge of the benefits of treatment for mental illness, I’d be skeptical with SGAs in adolescents and youth. I would prefer that they try different modalities first, but with my knowledge of mental illness, psychosis, and medications, I know it is more harmful to not treat psychosis and schizophrenia, and even more difficult to treat if there is a relapse in psychosis (Emsley et. Al., 2013). So, I don’t have any new questions but hopes to make these medications better with less side effects.
Emsley, R., Oosthuizen, P., Koen, L., Niehaus, D., & Martinez, L. (2013). Comparison of Treatment Response in Second-Episode Versus First-Episode Schizophrenia. Journal of Clinical Psychopharmacology, 33(1), 80-83. doi:10.1097/jcp.0b013e31827bfcc1
Nana,
You make a good point about the stigma associated with mental health in youth (at any age really) and as providers our responsiblity in normalizing their experience as well as normalizing medication as a part of their care. The difficulty in navigating adolescence, including peer pressure, puberty, and hormones, is only further compounded with the weight gain associated with SGAs; both the mental health challenges as well as increased weight gain can put youth at greater risk for being bullied, which only worsens their longterm mental health outcomes (Sigurdsen, Undheim, Wallander, Lydersen, & Sund). While the underlying mechanism causing weight gain is understood (Dayabandara, Hanwella, Ratnatunga, Seneviratne, Suraweera, & de Silva) I'm wondering if the sedation associated with these medication also makes weight gain prevention strategies more of a challenge; if one is sleepy most of the day exercise might not make the to-do list.
In working closely with adolescents and transitional aged youth, I have observed significant weight gain associated with second generation antipsychotics, however I am also currently monitoring a 21 year old on Zyprexa and Clozapine who is 6'1" and steady at 160lbs for the past 6 months - which is to hightlight that not everyone will gain massive amounts of weight on these medications, even when used in conjuction. Searching briefly on pubmed, I wasn't able to find anything if there is a compounded effect of multiple SGA's prescribed at once, however I'd be interested to know if the metabolic effects are further amplified with the combination of more than one SGA (e.g. is 2+2 is greater than 4). That said, weight gain is not something to trivilaize as a pesky side effect - it can seriously impact medication adherence, self-image, and quality of life.
References
Dayanbara, M., Hanwella, R., Ratnatunga, S., Seneviratne, S., Suraweera, C., & de Silva, V. (2017). Antipsychotic-associated weight gain: Management strategies and impact on treatment adherence. Neuropsychiatric Disease and Treatment, 13, 2231-2241.
Sigurdson, J., Undheim, A., Wallander, J., Lydersen, S., & Sund, A. (2015). The long-term effects of being bullied or a bully in adolescence on externalizing and internalizing mental health problems in adulthood. Child and Adolescent Psychiatry and Mental Health, doi:10.1186/s13034-015-0075-2
Lauren,
I am reading through all of these responses and your comment on concomitant antipsychotic use stood out to me. I, too, am curious whether or not the side effect burden is compounded when adding a second antipsychotic, but it is great to hear that your 21 year-old patient has not experienced weight gain! Does he have any other side effects such as increased sedation or hyperprolactinemia?
I just did a Google Scholar search on this topic, and found an older review on the risks and benefits of antipsychotic polypharmacy (Tranulis et al., 2008). As expected, the worsening side effects were related to the specific medication. Adding a second atypical antipsychotic onto risperidone worsened hyperprolactinemia, and adding a second antipsychotic onto clozapine worsened sedation. Surprisingly, I did not see much increase in weight gain amongst the studies presented in the review, which is reassuring. I wonder if anyone has some anecdotal experience to add on how side effects might worsen with adding a second antipsychotic to a patient's regimen? Thanks for a great discussion!
Reference
Tranulis, C., Skalli, L., Lalonde, P., Nicole, L., & Stip, E. (2008). Benefits and risks of antipsychotic polypharmacy. Drug Safety, 31(1), 7-20.
Hi Alexa,
While this is 100% anectodal, one of the youth I am following in clinicals is on the following medication regimen:
Cogentin 0.5mg BID
Celexa 20mg q/AM
Zyprexa 20mg QHS
Currently on a clozapine taper, this week we are at 400mg QHS and holding steady.
He has been on Celexa consistently since January, and Zyprexa intermittently since August of last year. Following his discharge from the hospital, we re-initiated his clozapine, as it was abruptly discontinued at John George as the inpatient unit MD's indicated that they could not support a medication taper at the hospital. That said, he has not experienced any weight gain in the past year, despite being on both Zyprexa and Clozapine. He sleeps approximately 12 hours per night, which he does not assess to be problematic for his lifestyle and level of functioning. During the day he does not complain of sedation or hypersomnia. The plan for him moving forward is to start peeling back the Zyprexa once stable on clozapine for at least a few weeks. Looking again to the literature regarding polypharmacy, it appears as though people who reduce the number of antipsychotic medications do best when the monotherapy remaining is clozapine (Constantine, Andel, McPherson, & Tandon, 2017). For his case, the addition of clozapine has significantly improved his level of functioning and motivation to continue treatment with minimal unwanted side effects.
Reference
Constantine, R., Andel, R., McPherson, M., & Tandon, R. (2017). Is the risk of antipsychotic polypharmacy discontinuation dependent on the agents used? Psychiatry Residence, 16, doi: 10.1016/j.psychres.2017.09.05
Lauren,
It is great he has not experienced weight gain on the combination. Though, he does seem to be the outlier, especially with olanzapine! It makes sense that when reducing concomitant antipsychotics, that clozapine is the best stand-alone therapy, given its strong anti-psychosis properties. I just wanted to share something I just came across when browsing the Carlat Report relevant to this discussion. A post titled, "Antipsychotic Polypharmacy: Helpful or Harmful?" It has some nice guidelines for cross titration/tapering of antipsychotics when used concomitantly.:
https://thecarlatreport.com/free_articles/antipsychotic-polypharmacy-helpful-or-harmful-free-article
Lauren,
You bring up a good point about the impact of SGA-induced sedation on physical activity. On one hand, we can choose SGAs that are less sedating - but sometimes, the sedation is a desirable effect, especially if the client has extreme behavioral dysregulation. If we have to use a medication that is heavily sedating, it might help to use a behavioral activation plan to ensure physical activity, and hope that it eventually becomes self-reinforcing as the routine exercise improves sedation and fatigue.
In addition to sedation, the negative symptoms of schizophrenia (which are significantly more debilitating than the attention-getting positive symptoms), especially avolition and anhedonia, make it very hard for clients to get regular physical activity, even if they wanted to. In this study, 38% of the male and 24% of the female participants had a schizophrenia diagnosis, but the study does not address their symptom severity, possible impact of negative symptoms (or sedation, for that matter) on their BMI changes.
Interestingly, according to one systematic review and meta-analysis of exercise interventions in adult patients with schizophrenia, rigorous exercise may not actually impact the BMI of patients with schizophrenia, but it does greatly improve functioning, co-morbid disorders, and neurocognition, and it improves general cardiometabolic risk factors and physical fitness (Firth et al., 2015).
References
Firth, J., Cotter, J., Elliott, R., & French, P. (2015). A systematic review and meta-analysis of exercise interventions in schizophrenia patients. Psychological Medicine, 45(7), 1343-1361. Retrieved from https://www-cambridge-org.ucsf.idm.oclc.org/core/journals/psychological-medicine/article/systematic-review-and-metaanalysis-of-exercise-interventions-in-schizophrenia-patients/1D5AAF2D1AEFE372541153F0D0DD37A3
Thanks for a journal club that offered some questions to ponder and reflect upon. Something that I started thinking about as a result from this journal club was in regards to when to implement things in practice that I read about in a journal article. This study, like many others out there, are small studies that yield statistically significant results, but may not yield clinically significant results. I am constantly struggling with this, whenever I read articles that are initial studies or studies that are small sample sizes. For example, this article suggested that perhaps we should intervene with SGA treatment if the patient gains 4% of their weight within the first month. While this is excellent food for thought, at what point does this become part of my practice? In this situation, it probably won't cause too many problems, because it is something that needs to be assessed with each individual case. But when it becomes part of our regular practice, but it's not yet considered "standard of practice" or the study is not yet a "landmark study", other practitioners may be quite confused with what you are doing.
One example I can think of is the intervention to start metformin prophylactically when starting a SGA to prevent weight gain/the progression to diabetes. There are studies out there that show that starting metformin (early) when starting an atypical can be beneficial (Hasnian, Vieweg, & Fredrickson, 2010; Jesus, Jesus, & Agius, 2015) to preventing metabolic syndrome and weight gain. While in theory this could make a lot of sense, in practice, this could cause a lot of problems. With the division of care, usually primary care manages diabetes and mental health specialists manage the mood disorder/psychotic disorder, or whatever the SGA is treating. If as specialists we start doing this as our standard of practice, it may be confusing to PCPs who would not typically start Metformin until they receive a diagnosis of diabetes. And if we somehow prevent diabetes, are we depriving the patients of certain care/resources they would have access to if they were "officially" diagnosed with diabetes and then started on Metformin later? And then there is the question of who follows and manages the Metformin when that is not in the PMHNP scope.
I don't have answers to the Metformin/SGA example above, but it makes me think about the transition between when research comes out that gives us promising information that could help our patients and when it becomes standard practice. Before things become standard practice, other practitioners may question our decisions and others may be confused about our decisions. I know we are weighing our decisions each time and taking the individual into consideration; of course we would not automatically switch the SGA if a youth gains 4% of their weight within the month if they are psychiatrically stable for the first time. But with the metformin example above, sometimes our decisions have a much wider impact than just switching an SGA.
Resources:
Jesus, C., Jesus, I., & Agius, M. (2015). A review of the evidence for the use of metformin in the treatment of metabolic syndrome caused by antipsychotics. Psychiatria Danubina, 27(1): 489-491.
Hasnain, M, Vieweg, W. V., Fredrickson, S. K. (2010). Metformin for atypical antipsychotic-induced weight gain and glucose metabolism dysregulation: review of the literature and clinical suggestions. CNS Drugs, 24(3): 193-206. doi: 10.2165.11530130-000000000-00000.
Madhubhashinee, D., Hanwella, R., Ratnatunga, S., Seneviratne, S., Suraweera, C., & de Silva, V. A., (2017). Antipsychotic-associated weight gain: management strategies and impact on treatment adherence. Neuropsychiatric Disease and Treatment, 13, 2231-2241.
Vandenberghe, F., Najar-Giroud, A., Holzer, L., Conus, P., Eap, C. B., & Ambresin, A. Second-Generation antipsychotics in adolescent psychiatric patients: Metabolic effects and impact of an early weight change to predict longer term weight gain. Journal of Child and Adolescent Psychopharmacology, 2017, 1-8. doi: 10.1089/cap.2017.0038.
Hi Sareen,
Thanks for sharing your thoughts! I think you honed in on the critical questions we'll all wrestle with in practice--when do we intervene and what do we do? Your point about clinical significance is well taken and it emphasizes the individualization of treatment for patients. The meta-analysis by Rummel et al. (2010) has a helpful summary RTCs on weight impact, glucose and cholesterol changes with amisulpride, aripiprazole, clozapine, olanzapine, quetiapine, risperidone, sertindole, ziprasidone and zotepine. The general results are in line with what we know, specifically olanzapine and clozapine resulted in greater weight gain and glucose increase than all other SGAs and olanzapine, amisulpride, clozapine and quetiapine increased cholesterol more than the others. They also point out trends in the effect of funding source on outcomes (something addressed in journal club) for the different studies on the different medications (generally studies funded by the manufacturer resulted in less significant increases) but also point out that the results are consistent (i.e., if a medication caused/was associated with weight gain in some of the studies it didn't ever cause/wasn't ever associated with weight loss in another study). Like you said, the assertion to intervene if a 4% gain in the first month is observed doesn't take into account the many other factors we're weighing. At the very least our awareness of the potential metabolic effects and the general timeline of when they are most likely to occur is useful and can give us additional information to consider. As far as who prescribes what, in my clinic psych doesn't prescribe "medical" meds but we do monitor metabolic parameters (weight, lipids, A1C) and work with primary care to address increases in them. Thanks for raising the questions you did; they're all great things for us to consider!
Rummel-Kluge, C., Komossa, K., Schwarz, S., Hunger, H., Schmid, F., Lobos, C. A., . . . Leucht, S. (2010). Head-to-head comparisons of metabolic side effects of second generation antipsychotics in the treatment of schizophrenia: A systematic review and meta-analysishttps://doi-org.ucsf.idm.oclc.org/10.1016/j.schres.2010.07.012
Hi Sareen,
You bring up an excellent point about when does a problem really become a problem, and how or when does this issue affect how you practice if there is no “standard of practice” to help guide the practitioner. I agree with you that there is extensive literature bringing up interesting areas of study, but how do we keep up as practitioners?
In my opinion if a pediatric client has 4% weight gain, which comes out to approximately 5 pounds, within a month of initiating SGA therapy, I would start monitoring that client closely. I think it is important to take into consideration other factors that may be contributing to the weight gain such as, female gender, low baseline BMI, young age, nonwhite ethnicity, and genetic variability (Vanderberghe et al., 2015). Also, once weigh gain has occurred we can add non-pharmacological interventions including behavioral interventions, changing to a more weight-neutral antipsychotic, or adding a pharmacologic weight loss agent (Krill, Kumara, 2014).
Also, not all SGAs necessarily cause weight gain, and we can always use a more weight neutral SGA, such as, aripiprazole which has the least weigh gain for a client we may be concerned about (Krill, Kumara, 2014).
If the client is stabilized on a particular SGA, it is difficult to switch to another SGA to prevent metabolic syndrome, but like you mentioned, maybe adjunct therapy such as, metformin would be suitable in some cases. As psychiatric np’s we have the authority to add adjunct medication to help alleviate side effects, and PCP may be onboard with our decision making.
Reference:
Krill, R.A., Kumra, S. (2014), Metabolic consequences of second-generation antipsychotics in youth: Appropriate monitoring and clinical management. Adolescent Health, Medicine and Therapies. 5, 171–182.
Vandenberghe, F., Gholam-Rezaee, M., Saigi-Morgui, N., Delacretaz, A., Choong, E., Solida-Tozzi, A., . . . Eap, C.B. (2015). Importance of early weight changes to predict long term weight gain during psychotropic drug treatment. Journal of Clinical Psychiatry. 76 (11), 1417-1423.
Reflect on your experience or knowledge regarding use of SGAs in adolescents or youth.
I don't have extensive experience prescribing SGAs to adolescents, however, I have experience working with adults who have been prescribed them for many years, some since adolescence. From my experience working with adults I know the side effects can significantly, negatively impact health. Unfortunately, I haven't seen great interventions for these negative effects. Of course minimizing medication, monitoring and lifestyle changes are all essential, but my patients often have limited capacity to engage in these lifestyle modifications. Monitoring at the clinic I'm at varies with more functionally impaired individuals monitored less frequently than the recommended monthly frequency (Pringsheim, Panagiotopoulos, Davidson, & CAMESA, 2011; Cooper & Reynolds, 2016). This is, of course, problematic because more impaired individuals likely have a more difficult time engaging in the behavioral/lifestyle interventions that can help mitigate negative metabolic effects. This further affects their quality of life and longevity. There is an especially urgent need to mitigate these adverse effects in children and adolescents because, presumably, they have a greater number of years over which to incur the negative and adverse health effects of the side effects of SGAs.
How does this article impact how you monitor adolescents or youth?
The article and information I've learned about the metabolic effects of SGAs has reinforced the importance of close monitoring of metabolic parameters in children and carefully considering the metabolic profile of different SGAs. I was also not aware that prescribing metformin was an effective and advisable intervention when lifestyle modifications are insufficient and switching medications is perhaps ill-advised.
Does this article trigger any new questions you have about SGAs in youth?
I've generally been hesitant to prescribe SGAs to children and psychotropics in general as all medications have costs associated with them. Certainly, there are situations when the costs of an illness outweigh the costs of medication and medication is effective and needed, but I think always carefully considering the metabolic impact of SGAs (and side effects generally of all medications), having a low tolerance for adverse side effects and taking measures to promote lifestyle changes that can mitigate the adverse metabolic effects are essential for providing the best care. As reported by Vandenberghe, Najar-Giroud, Holzer, Conus, Eap & Ambresin, (2017), initial weight gain appears to be related to overall and future weight gain, so paying specific attention to initial weight gain and modifying treatment (switching medications) in response to initially greater weight gain may help mitigate these effects. Based on the the readings, I would also initially prescribe SGAs with lower incidence of metabolic syndrome unless there was a clear and strong indication against it (Madhubhashinee, Hanwella, Ratnatunga, Seneviratne, Suraweera, & de Silva, 2017). Finally, I think it's easy to keep patients on medications without trialing decreased doses or working to minimize polypharmacy, but this is clearly important and something important to be consistently cognizant and reminded of.
Cooper, S. J. & Reynolds, G. P. (2016). BAP guidelines on the management of weight gain, metabolic disturbances and cardiovascular risk associated with psychosis and antipsychotic drug treatment. Journal of Psychopharmacology, 30(8): 717-748. doi: 10.1177/0269881116645254
Madhubhashinee, D., Hanwella, R., Ratnatunga, S., Seneviratne, S., Suraweera, C., & de Silva, V. A. (2017). Antipsychotic-associated weight gain: management strategies and impact on treatment adherence. Neuropsychiatric Disease and Treatment, 13, 2231-2241.
Pringsheim, T., Panagiotopoulos, C., Davidson, J., Ho, J., & CAMESA guideline group. (2011). Evidence-based recommendations for monitoring safety of second generation antipsychotics in children and youth. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 20(3), 218.
Vandenberghe, F., Najar-Giroud, A., Holzer, L. Conus, P., Eap C. B., & Ambresin, A. E., (2017). Second-Generation Antipsychotics in Adolescent Psychiatric Patients: metabolic Effects and Impact of a Early Weight Change to Predict Longer Term Weight Gain. Journal of Child and Adolescent Psychopharmacology. 20: 1-8. DOI: 10.1089/cap.2017.0038
While I’ve never prescribed SGAs to youth (I just started working with children in my internship), I have a lot of nursing experience with the use of SGAs in children. I spent several years working in a pediatric psychiatric hospital that included a 36-bed acute hospital and three residential treatment facilities (around 150 beds total) that specialized in sexual maladaptive behaviors, mental retardation/dual diagnosis (MRDD), and conduct disorders. As the nurse, I was responsible for doing the growth chart assessment on initiation and at regular intervals, tracking labs, monitoring and reporting side effects of medications, and providing patient and family education and obtaining consent from legal guardians. Because of the acuity of our clientele, we used a wide range of antipsychotics - the most common maintenance antipsychotics were probably risperidone and quetiapine (though we had a number of treatment-resistant patients on first-gen drugs like chlorpromazine), with olanzapine (oral or IM) the most common acute SGA. Weight gain was a frequent concern, but I recall the patients being much more distressed by other side effects like gynecomastia (especially with risperidone). Anecdotally, the MRDD clients were much more prone to developing type II diabetes and metabolic disorders - I’m not sure if this is due to genetic risk factors, higher likelihood of early initiation of antipsychotic therapy, higher doses needed to obtain desired outcomes, or a combination. My experience is limited by the institutional setting - all meals and snacks were controlled by a well-trained dietary team, so patients who may have had increased appetite with SGAs didn’t necessarily have access to all of the food they might have like to have eaten. In other hospitals I’ve worked in, providers would frequently order “double portions” to improve patient satisfaction and decrease conflict regardless of a client’s actual dietary needs, and weight gain was much, much more common.
This article gave me a chance to reflect on my prior experience, and to see the value of having a strong institutional culture of careful monitoring when prescribing any psychotropic. Providers should implement routing monitoring for relevant conditions, and carefully review the results at every visit. We also need to emphasize patient education, and recognize the patient as a partner in their health - they should be encouraged to help in risk-benefit analysis when it comes to choosing the right medication. This article demonstrates that the development of metabolic problems with SGAs follows a relatively predictable trajectory, so we don’t have an excuse for ‘watchful waiting’ as our young clients develop insulin resistance or other problems.
I think it’s important to remember that SGAs are not unique in their propensity for causing metabolic disorders, and many medications have potential for significant short- and long-term side effects (i.e. movement disorders) that can negatively effect our clients’ quality (and quantity) of life. It’s much easier to intervene in the early stages of weight gain, lab abnormalities, or movement disorders than it is to reverse those effects down the road.
Good article and good journal club discussion!
Another very exciting journal club! As we discussed, the topic is something that is relatively well known to us - weight gain with antipsychotics, but nonetheless research investigating this phenomenon is important. The authors tried to take a direction of creating guidelines as well, indicating when weight gain should be concerning and next steps. Though the conclusions of the article may be premature, this direction of research is exciting in that it can help to create more complete guidelines down the line when we are prescribing to children.
One thing we discussed that I really appreciated was the benefit of looking at the researchers when examining the study. This is something that I will use going forward as well - are the researchers known in the field already, is this a topic that they seem to be passionate about, or is this their first time publishing? Though it does not make or break the study, it can be an indicator of the rigor. When examining research, I find it important to look at it from as many angles as possible, and this adds yet another layer into this extremely nuanced process.
I have very little experience in prescribing to children/adolescents, so this article certainly got me started thinking. Though I do not think the benefits outweigh the side effects at this time for prescribing, I do think that it is important to pay close attention, as weight gain and metabolic syndrome can be life long for these patients. I think that when prescribing I will take the time to review diet with patients as well as stress the importance of monitoring. For all patients, I think there should be a bigger emphasis on nutrition and lifestyle education and support, as it is in this population that this can have the biggest impact.
Thanks for all of the substantive posts on this, they have really helped add to the multi-faceted nature of prescribing, especially to children/adolescents.
Vandenberghe, F., Najar-Giroud, A., Holzer, L. Conus, P., Eap C. B., & Ambresin, A. E., (2017). Second-Generation Antipsychotics in Adolescent Psychiatric Patients: metabolic Effects and Impact of a Early Weight Change to Predict Longer Term Weight Gain. Journal of Child and Adolescent Psychopharmacology. 20: 1-8. DOI: 10.1089/cap.2017.0038
The use of second-generation antipsychotics is well known in the field of psychiatry to cause weight gain. Specifically, the prevalence of cardiovascular diseases and conditions can be caused by a variety of factors, but those on antipsychotics have a large increase in weight gain due to the metabolic factors that antipsychotics have on the human body. From my experiences in working with adolescents, many of my patients have some sort of experience with SGA's. However, most of the presenting problems stem from behavioral issues in the home and/or school setting. For that reason, there is a good portion of children in my clinical practice who have yet to be prescribed an SGA. Like the article that was posted, the risks associated with hormonal-based weight gain in addition to an antipsychotic can be quite harmful to his or her health over a longer period of time.
Looking at some other research pertaining to this topic, some researchers believe that SGA's can be highly effective for acute psychiatric disorders for adolescents. However, even with such efficacy carries a risk like the posted article mentioned. Weight gain, sedation, EPS, elevated prolactin levels, and an increased risk of developing diabetes is much more pronounced within this specific age group (Kumra et al., 2007). It was suggested while clinical efficacy is important for stabilization, providers need to provide adequate education and the creation of a treatment plan to address these issues from the early onset of treatment as most of these conditions can gradually become chronic if left untreated.
Kumra, S., Oberstar, J. V., Sikich, L., Findling, R. L., McClellan, J. M., Vinogradov, S., & Charles Schulz, S. (2007). Efficacy and Tolerability of Second-Generation Antipsychotics in Children and Adolescents With Schizophrenia. Schizophrenia Bulletin, 34(1), 60-71. doi:10.1093/schbul/sbm109
I have limited experience in prescribing SGAs to adolescents or children. It was helpful to learn about the effects of SGAs on adolescents from this week’s journal club. Even in an adult, the metabolic side effects of SGAs are an important clinical factor to consider when prescribing and monitoring patients taking SGAs. Since adolescents or youth are going through puberty and hormonal changes, it is logical that the SGA weight gain side effect is much greater in adolescents relative to adults. I would imagine the long-term impacts of SGA therapy are more detrimental for this population both physiologically and psychologically (e.g., bullying, poor self-image). The article reminds me of the importance of patient education and close weight gain monitoring for adolescent or youth taking SGAs. The article triggers a new question about SGAs in youth: is prescribing metformin as an adjunct to SGAs a plausible way to prevent significant weight gain and the metabolic side effects from SGAs? I thought about metformin as a concomitant medication for adolescents on SGAs because it has a weight loss side effect, is a first-line of treatment for diabetes, is relatively safe to use, and potentially prevents the development of diabetes.
I reviewed a few research articles that I found via an online UCSF library and PMC search. I included three articles in this posting. Their conclusions about metformin therapy were not homogenous; however, two of the three I reviewed found a significant metformin benefit in preventing metabolic syndrome related to SGAs.
According to Webb & Viner (2006), metformin has shown small improvements in weight reduction for obese non‐diabetic adolescents with hyperinsulinemia. (Grade B); however, the efficacy and safety of long-term metformin use in children remains unknown. (Grade D).
In a meta-analysis of 12 published studies with a total of 743 patients who were on antipsychotics for schizophrenia or schizoaffective disorder, metformin was significantly effective in treating antipsychotic induced weight gain (Silva, Suraweera, Ratnatunga, Dayabandara, Wanniarachchi, & Hanwella, 2016).
According to Klein, Cottingham, Sorter, Barton, & Morrison (2006), a 16 week double-blind placebo-controlled trial study with 39 children and adolescents aged 10-17 years-old on atypical antipsychotics (e.g., olanzapine, risperidone, quetiapine) concluded that metformin therapy was safe and effective in treating antipsychotic induced weight gain, improved insulin sensitivity, and decreased abnormal glucose metabolism.
Thank you for the great discussion and an opportunity to dissect the article in depth as a group.
References
Webb, E., & Viner, R. (2006). Should metformin be prescribed to overweight adolescents in whom dietary/behavioural modifications have not helped? Archives of Disease in Childhood, 91(9), 793–794. https://ucsf.idm.oclc.org/login?url=http://doi.org/10.1136/adc.2006.098962
De Silva, V. A., Suraweera, C., Ratnatunga, S. S., Dayabandara, M., Wanniarachchi, N., & Hanwella, R. (2016). Metformin in prevention and treatment of antipsychotic induced weight gain: a systematic review and meta-analysis. BMC Psychiatry, 16, 341. https://ucsf.idm.oclc.org/login?url=http://doi.org/10.1186/s12888-016-1049-5
Klein, D., Cottingham, E., Sorter, M., Barton, B., Morrison, J. (2006). A randomized, double-blind, placebo-controlled trial of metformin treatment of weight gain associated with initiation of atypical antipsychotic therapy in children and adolescents. The American Journal of Psychiatry, 163(12), 2072-2079.
Thank you for posting a video, so that way the remote students are able to access the discussion in class and read the articles. I have to say that the articles we have been reading in this club have been very informative, and the information is useful for us in practice.
Reflect on your experience or knowledge regarding use of SGAs in adolescents or youth.
My only experience with adolescents or youth have been with Depression with Suicidal ideations in the emergency room. I rarely encounter encounter psychotic or adolescents with Schizophrenia in the emergency room, who are taking SGAs. I am familiar with the fact that most SGAs has the potential side effects of weight gain (mostly because I work with the adult population where there is significant weight gain), however, in adolescents I was shocked to see that SGAs can cause adolescents to have increase in weight gain that is 4% more than an adolescent who is not taking SGAs. The article this week, was very interesting to read, especially since the majority of SGAs used or recommended for adolescents are risperidone, zyprexa, and seroquel.
How does this article impact how you monitor adolescents or youth?
After reading the article, I did some more research and found some other articles that were interesting and informative as well. The impact of monitoring adolescents and youth on SGAs has brought a different perspective in how we will treat. I think a thorough past family medical history is need to be conducted, because we can then know how much the adolescent is at risk for metabolic changes. Also, a baseline lab work up will be necessary, as well as noting the dietary intake at home. One of the limitations in the article suggested that there wasn't information regarding the adolescent's dietary intake and exercise regime. Knowing this information will be helpful in treating adolescents, as well as educating their parents/caregivers.
The other important information we should consider is collaboration with the pediatric PCP of the adolescent. There was narrative review that discusses the most latest findings in regards to adolescents or youth taking SGAs (Pisano, et al., 2016). The article emphasized the importance of collaboration with the pediatric PCP, and active monitoring. Another important thing to remember is that not only weight gain and metabolic changes with SGAs, but there are also other SGAs, such as Geodon and others that can cause QTc interval prolongation (Pisano, et al., 2016). Therefore, we have to also consider cardiac concerns on top of metabolic changes, and be very thorough in monitoring adolescent patients who are taking SGAs.
Does this article trigger any new questions you have about SGAs in youth
I think the article was very enlightening and informative regarding SGAs and youth. I think that it brought up a lot of interesting information regarding management of SGAs in youth. Something that was interesting to note, and that I mentioned aboved was regarding dietary intake, and psychopharamco education provided to parents. It did not mention the lifestyles at home of the youth. Most youth and families these days have trouble preparing healthy meals and substitute fast foods for convienence and affordablity. I am wondering if education regarding side effects such as weight gain was addressed, was dietary modifications and exercise addressed as well? This is something to think about. Also, since there still needs to be more research involved regarding this information, I think its is important to wonder about these things and address them in future studies.References:
Pisano, S., Catone, G., Veltri, S., Lanzara, V., Pozzi, M., Clementi, E., … Masi, G. (2016). Update on the safety of second generation antipsychotics in youths: a call for collaboration among paediatricians and child psychiatrists. Italian Journal of Pediatrics, 42, 51. https://ucsf.idm.oclc.org/login?url=http://doi.org/10.1186/s13052-016-0259-2
I have no experience and a very limited knowledge regarding the use of SGAs in adolescents.
This article does impact how I would monitor my patients’ weight and the other side effects associated with SGAs. Like Yunji I was very curious about the metabolic changes associated with the SGAs. I knew SGAs affected weight but I didn’t realize that the metabolic changes could be so severe. However I did read an article that speculated that schizophrenia, and other brain disorders such as Alzheimer’s may be more closely linked to diabetes mellitus than previously believed. I could not find the exact article I read but searching for it I found some good research articles.
According to Bailey, Sharpe, Ringel, & Zeeshan (2018), collaborating with the patients’ primary care provider and mental health provider to monitor the patients’ blood sugar and metabolic syndrome, prevent serious complications, and adverse reactions. Providing a significant amount of education to the patient and their family is necessary, and appropriate. Drug naïve patients were associated with glucose dysregulation (Wani et al. 2015). Early detection of metabolic dysregulation is of the upmost importance when monitoring young patients prescribed SGAs.
The article did make me ponder some questions. Were the participants screened for genetic predisposition of diabetes or other metabolic disorders? Were the activity levels of the participants evaluated before the study to determine normal lifestyle habits, such as a sedentary lifestyle?
References
Bailey, R. K., Sharpe, D. K., Ringel, M., & Zeeshan, A. (2018). Early combination therapy for type 2 diabetes mellitus and common comorbid mental disorders. Foc, 16(1), 48-53. 10.1176/appi.focus.20160048 Retrieved from https://ucsf.idm.oclc.org/login?url=https://doi.org/10.1176/appi.focus.20160048
Wani, R. A., Dar, M. A., Margoob, M. A., Rather, Y. H., Haq, I., & Shah, M. S. (2015). Diabetes mellitus and impaired glucose tolerance in patients with schizophrenia, before and after antipsychotic treatment. Journal of Neurosciences in Rural Practice, 6(1), 17-22. 10.4103/0976-3147.143182 Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4244781/
SGA use carries the risk of weight gain. With the increase in weight gain, runs additional risk of developing type 2 diabetes and cardiac complications. Use of SGA's in adolescents further increases their risk due to undergoing puberty. The addition of hormones to promote growth in conjunction with side effects from SGA can increase the risk of the adolescent developing secondary health complications as an adult. Adolescents also have less control of their dietary intake due to reliance on adults and schools for their meals. If the parents are not feeding the adolescent nutritiously balanced meals, it would be difficult to attribute weight gain to use of SGA's.
I feel that if a SGA is able to successfully reduce psychiatric symptoms, it would be appropriate to continue its' use. The healthcare provider should continue to monitor weight with every visit and perform routine labs.
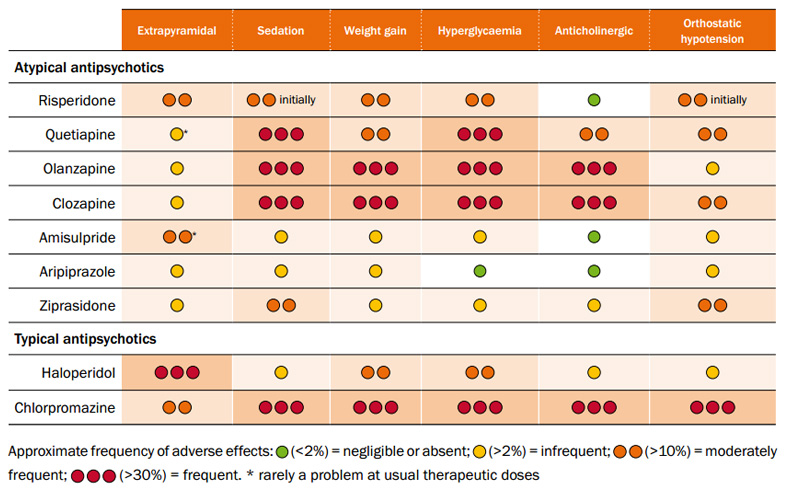
Below is a good chart to list psychotropic medications with cause weight gain.

Thank you Yacharter for your post,
I especially liked the point that was brought to light concerning adolescent having less control of their dietary intake, and rely on others such as parents, guardians, and/or schools for their meals. If these systems are not feeding them responsibly and supplying nutritiously balanced meals, then it would be difficult to attribute the entirety of weight gain on SGA’s. Seth brought out in discussion, care givers need to be educated not only on adverse effects of SGA’s, but also on proper nutritional/dietary needs of these youths while taking these medications. If benefits out weight risks, then continued use is warranted. According to (Strassnig, Brar, & Ganguli,2005) physical health risks of excess body weight are numerous and include, insulin resistance, DM, and hyperlipidemia. However, obesity also contributes to other physical disfunctions as well such as; sleep apnea, chronic hypoxia, hypercapnia, degenerative joint disease, certain cancers, as well as gall bladder disease. Many of these disorders begin as early as adolescence and continue into adulthood which bring many disparities to their victims. Proper nutrition while on SGA’s are an important reality and need to be addressed by caregivers to minimize the effects of possible obesity. Also, schools and other institutions of learning need to be educated on adolescent nutritional needs while they are on SGA’s.
Thanks again for an exceptional post.
Reference:
Strassnig, M., Brar, Jaspreet, & Garguli, Rohan. (2005). Dietary intake of patients with schizophrenia. Psychiatry MMC, PCID:PML3O04718
Hey Charter,
I like the chart you posted. I also found this chart to be very helpful regarding SGAs medications. However, even if we have adolescents patients taking SGAs, we can assist them to prevent weight gain. We can work together with the PCP, and work on a treatment plan to prevent or reduce weight gain, such as dietary counseling, exercise, etc. I think we will have to collaborate together with other disciplines to provide adequate care.
REFERENCE:
Prescribing atypical antipsychotics in general practice. (2011). Retrieved March 11, 2018, from https://bpac.org.nz/BPJ/2011/november/antipsychotics.aspx
Thank you for your post, Yacharter,
You bring up an good point which is that kids and adolescents do not have much control over their dietary intake due to their reliance on adults for their meals. In light of the journal club article, this really speaks to the importance of providing psychoeducation to caregivers regarding healthy weight management in youth taking antipsychotics.
Looking through the literature on this topic, I found a 2016 study in Childhood Obesity that surveyed the parents of overweight children/adolescents taking antipsychotics. The questionnaire sought to understand the caregivers' self-perceived barriers and preferences regarding weight loss in their overweight children.
The researchers found a number of things relevant to our practice as NPs. Firstly, they found that parents were generally quite motivated to help their kids lose weight, but tended to lack the time and resources to do so. They point to the role of telemedicine to improve access to care and also suggest teaching parents about smart phone apps to help with monitoring and tracking of their children's food intake and exercise.
Parents also reported that their children tended to not enjoy traditional forms of physical activity, which they attribute to the underlying mental illnesses for which they were prescribed antipsychotics. To address this, the authors also suggest use of apps and games that encourage physical activity and movement and can easily be used in various settings, such as at home.
They also found that children strongly prefer highly caloric foods, and that parents reported wanting more help with shopping lists and individualized meal plans to help make healthier meals for their kids.
Lastly, they found that providing referrals to weight management programs and actively discussing concerns about weight gain in practice was helpful, as participants were far more likely to get help with weight loss when referred as opposed to seeking out support on their own.
Nicol, G., Worsham, E., Haire-Joshu, D., Duncan, A., Schweiger, J., Yingling, M., & Lenze, E. (2016). Getting to more effective weight management in antipsychotic-treated youth: a survey of barriers and preferences. Childhood Obesity, 12(1), 70-76.
Although, I have never prescribed SGAs before, I have administered SGAs countless number of times to both youth and adults. I have had extensive experience as a RN working with both youth and adults in a variety of psychiatric settings such as, juvenile hall, jail/prison, group homes, inpatient psychiatric units, and county psychiatric health facility (PHF), also known as the county “Puff”. The reason I mention this work experience is that I have first hand, seen the effects of SGA’s on both populations.
Through my own personal assessment over the years, increased weight, diabetes, and high blood pressure were notable in a short period of time in the adolescent population in comparison to the adult population. Although, there are many risk factors that exacerbate metabolic syndrome (Mets) quicker in some than others such as, genetics, family history, and lifestyle (Vandenberghe et al., 2017). My personal hypothesis was that since the adolescent body is changing rapidly, that their bodies are more sensitive to SGA’s than an adult. It appears that Vandenberghe et al. (2017) mentions this is a reason Mets is seen quicker in the pediatric population as well (Vandenberghe et al., 2017).
It was very disheartening seeing pediatric patients struggle with severe mental illness and their quality of life suffering. As we were treating their mental illness, I felt terrible knowing we are exposing them to detrimental health problems that can exacerbate their mental health condition in the long run.
For example, weight gain for an adolescent, especially adolescent female is particularly sensitive since they are constantly bombarded with images of unrealistic females via social media, tv, and magazines, and the pressure to meet those standards. Also, the adolescent period is a time of trying to figure oneself out and “fit” in with peers and becoming interested in pursuing relationships. Many times, low self-esteem contributes to feelings of depression and social isolation. Some kids refuse treatment due to weight gain and begin decompensating, and the vicious cycle continues.
As a nurse, I felt moral distress, lacking power or authority to make decisions, and knowing that SGAs have many side effects, but that the benefits outweigh the risk, and keeping the child safe is a priority (Ohnishi et al., 2018).
After reading Vandenberghe et al. (2017), it is comforting to know that there is literature providing evidence of SGA side effects and cautioning providers to pay close attention to at risk patients (Vandenberghe et al., 2017). Vandenberghe et al. (2017) offered other solutions such as, behavioral interventions, diet, and physical activity in conjunction to SGAs, which allows providers to try different methods in treating adolescents (Vandenberghe et al., 2017).
Being in a prescribing/provider role in the near future, I feel I will be more cognizant of how I will prescribe SGAs. At the same time, I will keep in mind that SGAs are important when initially stabilizing a patient and keeping them safe, however I will choose more weight neutral SGAs for high risk Mets patients and offer other therapies adjunct to medication therapy.
Reference:
Ohnishi, K., Kitaoka, K., Nakahara, J., Va¨lima¨ki, M., Kontio, R., & Anttila, M. (2018). Impact of moral sensitivity on moral distress among psychiatric nurses. Nursing Ethics. https://doi-org.ucsf.idm.oclc.org/10.1177/0969733017751264
Vandenberghe, F., Najar-Giroud, A., Holzer, L., Conus, P., Eap, C.B., & Ambresin, A.E. (2017). Second generation antipsychotics in adolescent psychiatric patients: Metabolic effects and impact of an early weight change to predict long term weight gain. Journal of Child and Adolescent Psychopharmcology, XX(XX), 1-8.
Shararah, I am so glad you mentioned the moral distress involved with administering SGAs as a nurse. It made me consider how moral distress plays a part in the settings you have worked in (where an MD prescribes and an RN administers) compared to my clinical site and similar settings (where the prescriber also administers the injection --- we don’t have RNs). I have definitely experienced moral distress at my clinical site, as I am following several TAY patients who are on oral or LAI SGAs with subsequent severe weight gain. My supervising psychiatrist is officially prescribing these medications, but I am administering them and will soon be prescribing them.
Under the psychiatrist’s supervision, I’ve also been starting patients on Metformin, ordering labs for metabolic monitoring, tracking patients’ weight, and trying my best to offer practical nutrition and wellness counseling. I have seen significant improvements in some patients’ psychotic and/or mood symptoms, but I am now witnessing severe weight gain and metabolic disturbances. In my clinical setting, the SGAs that are currently causing these side effects are clozapine, aripiprazole, and palliperidone.
Like you, I hope to use SGAs that are more likely to be weight-neutral when treating children and adolescents. Unfortunately, our choices are limited. I still hear people say aripiprazole is weight neutral, but that hasn’t been my experience and it doesn’t seem to be supported in the literature, particularly for children and adolescents (Goltz & Rice, 2017).
I think the issue of SGAs and metabolic disturbances will continue to create moral distress and challenge us to be astute providers who approach patient care holistically with an emphasis on wellness and prevention.
References:
Goltz, J. S., & Rice, T. R. (2017). Commentary: A Randomized, Double-Blind, Placebo-Controlled Trial of Metformin Treatment of Weight Gain Associated with Initiation of Atypical Antipsychotic Therapy in Children and Adolescents. Frontiers in Psychiatry,8. doi:10.3389/fpsyt.2017.00059
Vázquez-Bourgon, J., Pérez-Iglesias, R., Foz, V. O., Pinilla, P. S., Martínez, Á D., & Crespo-Facorro, B. (2017). Long-term metabolic effects of aripiprazole, ziprasidone and quetiapine: A pragmatic clinical trial in drug-naïve patients with a first-episode of non-affective psychosis. Psychopharmacology,235(1), 245-255. doi:10.1007/s00213-017-4763-xI enjoyed reading everyone's posts related to SGA use in adolescents. I thought that all of you brought up good points that are important pieces of the conversation. In my clinical site, I see children and adolescents one day a week and I really haven't seen a lot of clients who take SGAs. Because of their side effect profile, we do not use them very often. Additionally, most of our clients are being seen for depression, anxiety, and/or PTSD and are on SSRI's. However, my preceptor and/or I see a few clients on SGA's and I have found that there is some focus on weight gain, but that this side effect deserves more attention. For example, my preceptor saw a client yesterday who is taking Abilify. He is overweight and has gained a few pounds since being on the medication, however, my preceptor and I spoke and this client's hallucinations are so distressing for him that my preceptor decided to increase the dose of the abilify. I think that side effects like weight gain can be such a difficult symptom to manage especially since the effects are more downstream instead of immediate. When do we decide to draw the line and change medications? I worked with the client and his mother around nutrition and physical exercise, but the client's father refuses to come into sessions and the client lives with him 50% of the time. One of my peers already mentioned this difference between working with children and working with adults, children are not always involved with the family meal planning so it is important to involve the family in these discussions. However, in my case and in many other of my clients, one parent is more invovled than the other and it makes it difficult to construct a plan that best meets the needs of the client. I appreciated this article because it helped give me a framework to manage my client's symptoms/side effects and I enjoyed learning from everyone on this thread about their experiences with these medications.
Reflect on your experience or knowledge regarding use of SGAs in adolescents or youth.
How does this article impact how you monitor adolescents or youth?
Does this article trigger any new questions you have about SGAs in youth?
I have been doing my internship in a county mental health clinic for children and adolescents, so I have some growing experience with the use of SGAs in adolescents and transitional-age youth. I will be working with transitional age youth very soon, so I am quite interested in the metabolic risks of SGAs in this population.
Unfortunately, unlike the baseline rate of obesity reported in the population used in the study we read for this session, many of the youth whom I or my preceptors have started on an SGA already had high BMIs. This is one reason why obtaining baseline metabolic lab studies is very important prior to starting treatment, and comparing these to results obtained over time. I recall two young, underweight men for whom we prescribed quetiapine, purposefully employing the side effects of weight gain and sedation in their favor. However, these patients will still need to be monitored at least yearly for metabolic changes and at each visit for excessive weight gain.
We know that second-generation antipsychotics increase the risk for metabolic syndrome (MetS) However, we cannot tell a specific patient on a specific SGA that after specific length of time on said SGA that they have a specific numerical risk of MetS or a certain expected rate of weight gain. Furthermore, patients enter treatment with varying levels of predisposing risk for diabetes and atherosclerotic heart disease. Thus, all patients should be counseled, using the MI approach, and every visit, about diet and physical activity. My concern with my youth is that they may possibly be on SGAs for a long time,
I went to a psychiatry conference last September and heard a presentation on metabolic syndrome and antipsychotics (unfortunately I cannot provide a reference as I did not purchase the slides and therefore do not have the speaker's name or even the title of the presentation). This speaker confirmed what Vandenberghe et al (2018) reported: namely, that weight gain early into treatment with SGAs is prognostic of risk for developing MetS in the future. We know from the CATIE trial that rates of continuous treatment for 18 months is very low for all antipsychotics studied , ranging from 18% for quetiapine to 36% for olanzapine. (Chen, McCombs, and Park, 2007). Subsequent studies have found similar rates of discontinuation (Chen, McCombs, and Park, 2007). Anecdotally, medication adherence is a big issue for all patients, but youth seems to pose additional threats to adherence. Therefore, if I see a 4% weight gain in a given adolescent patient on quetiapine within 3 months, I will counsel them on weight management and the risk for MetS, but I may not have high expectations that they will still be taking quetiapine in a year. I think that it is important to mindfully consider the risks and benefits of starting an SGA on a young person in the first place (especially for indications other than severe mental illness). Once on an SGA, it is important to approach the issue of metabolic syndrome holistically and individually for each patient.
The question I am left with has to do with the duration of pharmacotherapy with an SGA and risk for MetS. The Vanderberghe retrospective study did not control for whether or for how long subjects had been on the antipsychotics, which I felt was a huge limitation. So, if I initiate quetiapine on a 16-year old male, and he takes it for 7 months and then self-discontinues it, does that length of treatment increase his lifetime risk of MetS independently of other risk factors he may have? This question is less salient if he has clear-cut schizophrenia or bipolar disorder (where the risks of the untreated illness may outweigh the risks of the medication) but what about in cases that I see often, where quetiapine is being used to target anger or insomnia primarily, with a BAD on the differential?
References:
Chen, L., Mccombs, J. S., & Park, J. (2008). Duration of Antipsychotic Drug Therapy in Real-World Practice: A Comparison with CATIE Trial Results. Value in Health, 11(3), 487-496. doi:10.1111/j.1524-4733.2007.00262.x
Vandenberghe, F., Najar-Giroud, A., Holzer, L., Conus, P., Eap, C. B., & Ambresin, A. (2018). Second-Generation Antipsychotics in Adolescent Psychiatric Patients: Metabolic Effects and Impact of an Early Weight Change to Predict Longer Term Weight Gain. Journal of Child and Adolescent Psychopharmacology. doi:10.1089/cap.2017.0038
Reflect on your experience or knowledge regarding use of SGAs in adolescents or youth.
I have been working with severely mentally ill TAY during my second year of the PMHNP program and I’ve had the opportunity to closely follow/monitor an 18 year old male patient (CP) who was started on clozapine during his most recent hospitalization in late November 2017. Although none of the participants in the study were taking clozapine, it is one of the worst SGA metabolic offenders, so is quite relevant. CP was diagnosed with schizophrenia in late 2016 and has been hospitalized four times since then. Negative and catatonic symptoms are particularly debilitating for CP and he had minimal, if any, response to po olanzapine and IM aripiprazole, which is why he was started on clozapine during his 4th hospitalization.
CP has experienced significant improvement in his catatonic symptoms since starting clozapine, but he is still impaired by negative symptoms as well as regular auditory hallucinations. He has gained 32 lbs in 3 months, which is nearly 20% of his baseline weight of 164 lbs. Thankfully, CP’s lipid panel and HbA1c are within normal limits. We started him on Metformin 1000 mg/day about 45 days after he started on clozapine due to severe weight gain and to help prevent insulin resistance. I should also mention that CP experiences several other bothersome side effects of clozapine, but he continues to take it with the support of his family who fear for his health and safety if he is non-adherent.
My experience with CP has been incredibly challenging and eye-opening. I have been struggling to help him find creative ways to improve his diet and increase his level of physical activity. His negative symptoms seem to interfere with his ability to understand and/or implement small dietary and physical activity changes and his family’s living and financial situation make it even more difficult. Access to healthy food and safe options for physical activity are scarce due to these factors.
I’ve had some exposure to SGAs being prescribed to younger children for violent/disruptive behavior (primarily Risperdal) and noticed inconsistent metabolic screening practices among prescribers. I have also seen significant metabolic disturbances in a very short amount of time in younger children, which is likely to jeopardize their future health, as mentioned in the article.
How does this article impact how you monitor adolescents or youth?
Because of my clinical experience as a PMHNP intern, I plan to follow established guidelines for metabolic monitoring for all of my future patients on SGAs and to be very upfront with patients (and their parents when required/appropriate) about side effects and plans for monitoring. Some of the barriers to consistent metabolic monitoring are logistical considerations such as transportation to and from the lab, scheduling conflicts, fasting considerations, and long wait times at the lab. If resources are available at my future workplaces, I plan to utilize case management/care coordination services to help address these barriers. Even without additional resources, I plan to discuss barriers with patients and their families and help problem-solve to address them.
Does this article trigger any new questions you have about SGAs in youth?
I have a strong interest in the metabolic effects of SGAs in patients of all ages and interventions to consistently monitor for and treat subsequent metabolic disturbances. My comprehensive exam will explore existing research on the subject! One of the questions that I hope to answer through my literature review is whether or not there is a clinically meaningful difference in metabolic monitoring rates between psychiatric prescribers and primary care providers.